Acute stroke Treatment
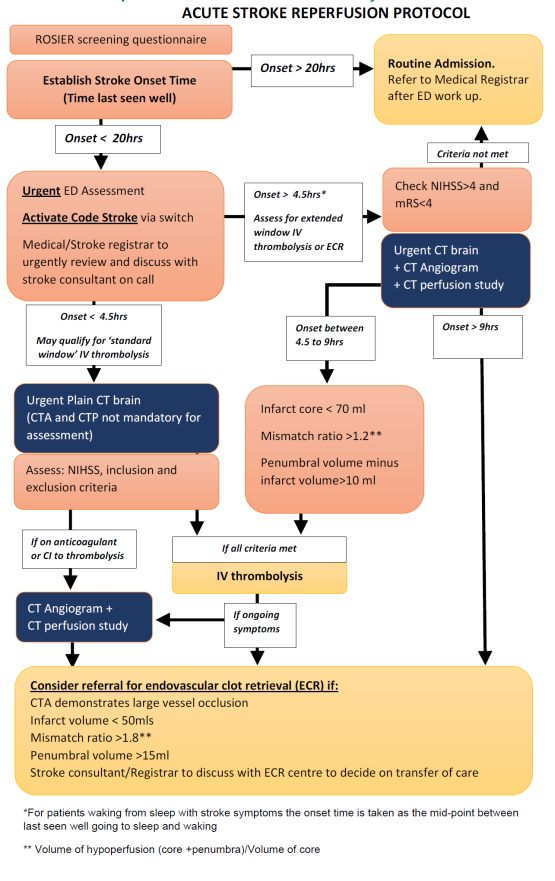
Thrombolysis Protocol
Inclusion criteria
•
Clinical
diagnosis of stroke (NIHSS >/= 4 or less than 4 when clinically relevant -
dysphasia, visual field defects)
•
Patient’s
head CT scan does not show haemorrhage or non-vascular cause of stroke symptoms
•
Patient’s
age is >18 years
Exclusion
criteria
|
ABSOLUTE
Contraindications |
Details/Timeframe |
|
Acute
Intracranial haemorrhage |
|
|
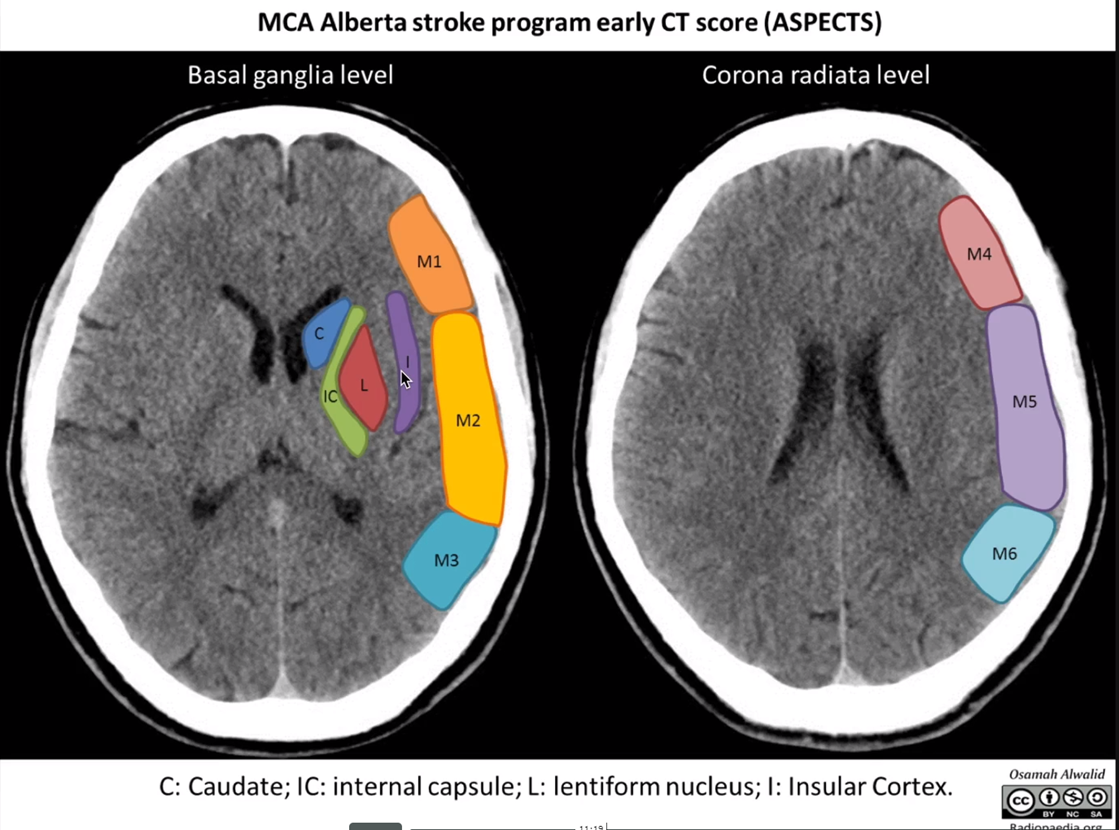
CT
evidence of extensive middle
cerebral artery territory infarction |
(sulcal
effacement or blurring of grey-white junction in >1/3 of middle cerebral
territory or ASPECTS <6-7) |
|
Active,
non-compressible systemic bleeding |
|
|
Platelets
<100 |
|
|
Heparin
(and elevated APTT) |
48 hours |
|
LMWH
(treatment dose) |
24 hours (Consider
measuring anti-factor Xa activity) Prophylactic
dose not absolute CI |
|
DOAC |
48 hours |
|
Known hereditary
or acquired haemorrhagic diathesis |
|
|
Presumed
septic embolus/infective endocarditis |
|
|
Stroke
secondary to aortic dissection (cervical artery dissection is not CI) |
|
|
RELATIVE Contraindications |
|
|
Hypertension ≥185/>110 mmHg |
|
|
Pre-existing severe disability (MRS >/=4) |
|
|
History of: ·
intracranial haemorrhage ·
SAH ·
intracranial AVM ·
known intracranial neoplasm |
|
|
Ischaemic stroke |
3 months |
|
Major surgery |
14 days |
|
Lumbar puncture |
7 days |
|
Cranial or spinal surgery |
3 months |
|
Major head trauma |
3 months |
|
Hypo or hyperglycaemia |
<3.0 mmol/L or >22.0 mmol/L |
|
Pregnancy |
|
|
Gastrointestinal or urinary tract haemorrhage |
21 days |
|
Transmural myocardial infarction |
30 days |
|
CPR |
7 days |
|
Arterial puncture at non-compressible site |
7 days |
|
Seizure at onset |
(with normal perfusion scan/CTA) |
Note, the following ARE NOT
contra-indications to thrombolysis:
•
Recent
TIAs (deficits fully resolved)
•
Prior aspirin
or clopidogrel use
•
Meningioma
•
Unruptured
cerebral aneurysm
Hypertension management
No benefit in
treating BP unless candidate for thrombolysis
Prior to
thrombolysis aim for BP <185/110
Suggested
medications:
• Labetalol 10-20mg IV (over 1-2min, repeat in 10-15min)
o Continuous IV infusion 0.5-3mg/min
• Metoprolol 2.5-5.0mg IV (1-2mg/min, repeat after 5 min)
• Hydralazine 5-10mg IV (repeat after 20-30min)
o Continuous infusion200-300mcg/min then maintenance 50-150mcg/min)
• GTN infusion (50mg in 500ml N/Saline)
DOACS
Treatment with a DOAC in general still precludes thrombolysis (can still consider ECR)
There is some evidence that thrombolysis is safe after reversal of dabigatran (Theodorou, et al. Thrombolysis After Dabigatran Reversal for Acute Ischemic Stroke: A National Registry-Based Study and Meta-Analysis. Neurology. 2024;103(7):e209862.
•
Dabigatran
o Idarucizumab (2 x boluses of 2.5g (50ml) no more than
15 min apart)
Thrombolysis medication
Alteplase
Dose is 0.9mg/kg (maximum dose 90mg) given as:
•
10% of
total dose given as a bolus over 1 minute
•
the
remaining 90% as an infusion over 60 minutes
•
100 mls of normal saline at end of dose to ensure the full dose
of alteplase is administered
•
When
mixing pierce the water first, then put power on top,
then invert to mix.
Tenecteplase
• Total dose = 0.25 mg/kg (maximum 25mg (5mL) given as bolus over 10 seconds).
• Flush the line before and after injection to avoid precipitation in the line.
• N.B. Cardiac dose is different – confirm that stroke dose is being used.
Post-lysis management
•
No
antiplatelet or anticoagulant agents to be given for 24 hours after treatment
•
Placement of NG tubes, urinary catheters,
venepuncture or other invasive procedures should be avoided.
•
Obtain
blood from IV bung if possible. If venepuncture is required, apply direct
pressure for 20 minutes
•
BP
should be maintained at <185 systolic and <110 diastolic for 36 hours
following alteplase treatment
Managing Complications
If ICH or systemic haemorrhage:
• Cease infusion
• Check bloods
• Consider cryoprecipitate
5-10 units (1 unit/10kg body weight)
Angioedema
• Promethazine
12-25mg IV Q6-8 hours
• Hydrocortisone
100mg IV Q6 hours
• Ranitidine 50mg IV
Q8 hours
• DO NOT GIVE
ADRENALINE (may increase BP and precipitate bleeding)
Pathophysiology
·
Every
10min, 20million neurones will die in a typical infarct in the MCA territory
(Lancet 2010, 375:1667)
Outcomes
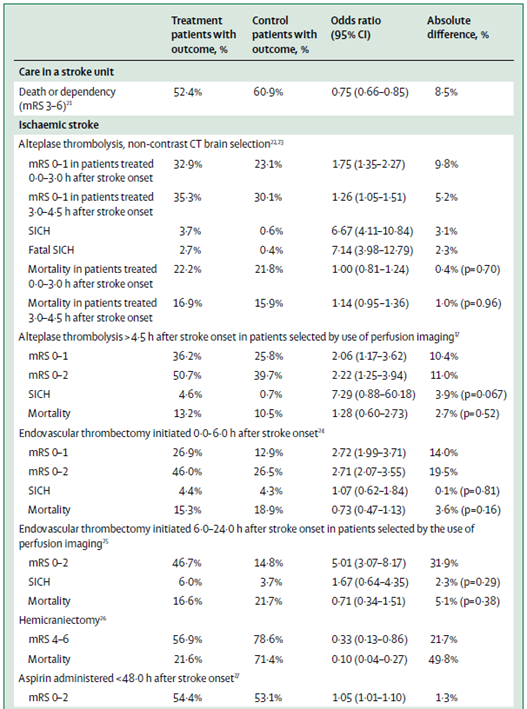
(Campbell BCV, Khatri P. Stroke. Lancet. 2020;396(10244):129-142)
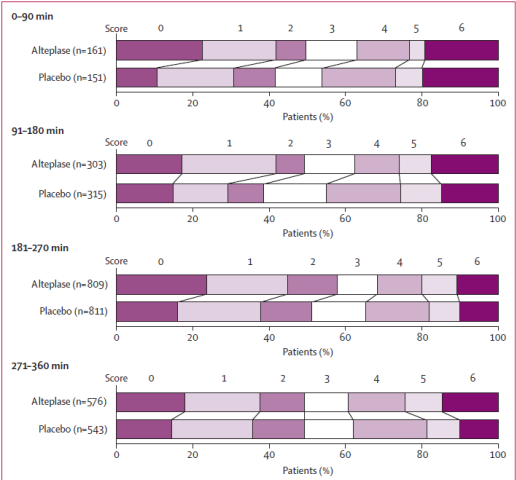
From Lancet 2010
combined results:
Modified Rankin 0-1
at 90days
|
Time (min) |
OR |
ARR |
NNT |
|
0-90 |
2.55 |
4.5 |
|
|
91-180 |
1.64 |
9.0 |
|
|
180-270 |
1.34 |
14.1 |
|
|
271-360 (not signif) |
1.22 |
21.4 |
|
|
0-360 |
1.4 |
12.6 |
Risks
Intra-Cranial
Haemorrhage
·
Factors
associated with risk of haemorrhage include:
o Age
o Established infarct on initial CT
o
Treatment
delay and premorbid function of borderline significance
Other systemic haemorrhage
Angioedema
Mortality
·
Overall
data OR 1.17 (NS)
·
Australian
data OR1.04 (NS)
·
May be
a higher death rate in first two weeks which is balanced out with better
survival in remainder such that by 3 months roughly equal.
Cochrane
meta-analysis
·
OR for
death or disability 0.8
·
Equivalent
to 55/1000 additional independent survivors
Imaging
ASPECTS Score