EEG
Technical
Electrodes
• Made from gold or silver (or compounds thereof)
• Skin abrasion prior to application
• Attached with electroconductive substance
o Gel
o Collodian
- Dries hard for long lasting attachment
- Requires acetone for removal
- ?Potentially teratogenic – avoid use in pregnancy
• Impedance should
be less than 5 kOhms
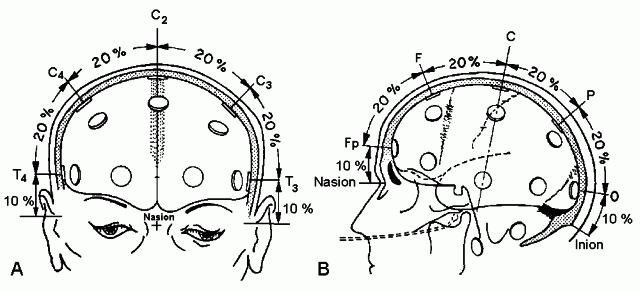
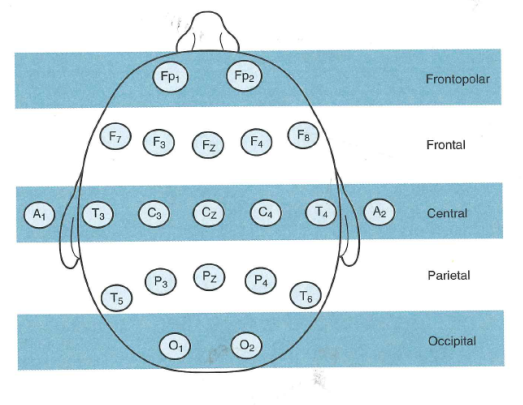
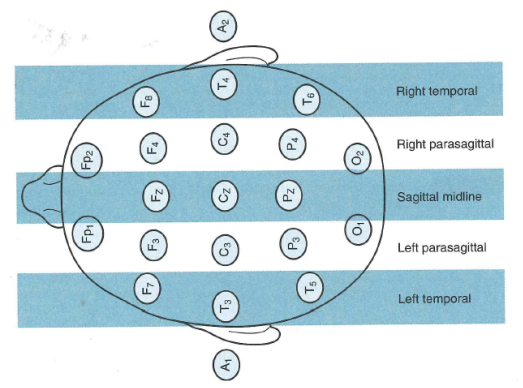
Electrode Placement
• 10-20 system
o Measured from nasion at front and inion at back
o Measured from tragus of ear on each side
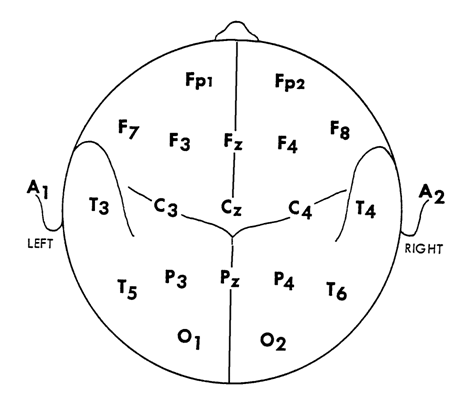
Lead descriptions
|
Lead |
Description |
|
Fp1 and Fp2 |
Frontopolar |
|
F7 and F8 |
Anterior temporal (or frontal) |
|
F3 and F4 |
Superior frontal (or midfrontal) |
|
Fz |
Frontal midline |
|
T3 and T4 (T7, T8) |
Midtemporal |
|
C3 and C4 |
Central (Rolandic) |
|
Cz |
Vertex or central midline |
|
T5 and T6 (P7, P8) |
Posterior temporal |
|
P3 and P4 |
Parietal |
|
Pz |
Parietal midline |
|
O1 and O2 |
Occipital |
|
Sp1 and Sp2 |
Sphenoidal |
|
A1 and A2 |
Ears |
Filters
Time constant = R x C
R = resistance
C = capacitance
Time constant is the amount of time to reduce high frequency waves by
63% or low frequency by 37%
It should be noted that digital filters do not use resistor/capacitor
circuit and use digital filters
Digital processing
Nyquist theorem
Required sampling rate = 2 x fmax
This will only sample a wave twice – so in reality to properly represent
a wave this needs to be further multiplied by 2x-5x
Most machines have a sampling rate of att least 200Hz ( and so can
accurately represent 50Hz and below)
Montages
Referential
Bipolar
• When input 1 is negative compared to input 2 – upward (negative) deflection
• When input 1 is positive compared to input 2 – downward (positive) deflection
|
Input 1 |
Input 2 |
Deflection |
|
Neg |
- |
Upward (Negative) |
|
Pos |
- |
Downward (Positive) |
|
- |
Neg |
Downward (Positive) |
|
- |
Pos |
Upward (Negative) |
LINEUP (Lead 1 – Negative – Up)
|
Referential |
Good for assessing symmetry Avoid electrode cancelling |
Reference can be involved/contaminated by
discharge |
|
|
Average |
|
|
|
|
Source (Laplacian) |
|
|
|
|
Ipsilateral Ear |
|
Electrodes are variable distance from
reference Temporal activity can contaminate reference |
|
|
Contralateral Ear |
Does not have problem of contamination of
ipsilateral temporal contamination |
Electrodes are are very long and variable
distance from reference |
|
|
Vertex |
|
|
|
|
Bipolar |
|
Lead will not register response if large
area area of discharge End of chain issues |
|
|
|
|
|
|
Normal EEG
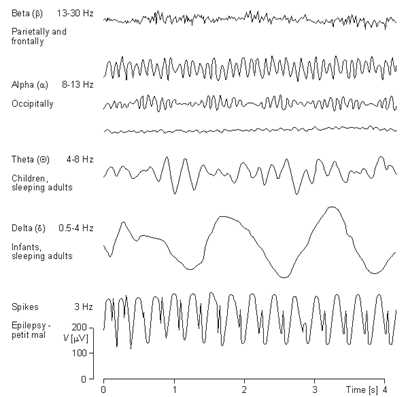
Frequencies
|
Name |
Frequency |
Notes |
|
Delta |
1-3Hz
(<4Hz) |
High amplitude, slow |
|
Theta |
4-7Hz
(<8) |
|
|
Alpha |
8-13Hz* |
Posterior regions Occur with eye closing and relaxation Present during most of life |
|
Beta |
>13 Hz- 25Hz |
Mainly frontal Normal rhythm in most awake people with eyes
open. |
|
Gamma |
>25Hz |
(Controversial term) |
* The alpha band is the only one to include the upper boundary
frequency. i.e. It includes 13 (but not
13.1)
Background frequencies
Alpha
• Posterior dominant
• Attenuates with eye opening
• Is bilaterally absent in 5% of people
• Unilateral absence is pathological - indicative of complete dysfunction of underlying brain (e.g. infarction)
• If a person in very tense alpha will be will evident
• If a person is drowsy then alpha will be more common – may also be present more frontally
• Dementia states can result in more universal alpha
• Slow alpha variant – normal variant (see below)
• Asynchrony
o Up to 1Hz difference in alpha frequency is allowable between sides
• Alpha symmetry
o The amplitude of right sided alpha is usually ~20% higher than left.
o For asymmetry to be abnormal:
- Left amplitude >2x right (= right <50% of left)
- Right amplitude >3x left (= left <33% of right)
Beta
• Normal background rhythm
• Predominant in fronto-central regions
• Does not attenuate with eye closure
• Asymmetrical beta is sign of underlying brain dysfunction
Theta
• Present in normal EEG’s however in general should not be present in >5% of waking adult trace
• More predominant with drowsiness – seen in the occipital and temporal regions in particular
• Can occur in rhythmic, hypersynchronous runs during drowsiness (hypnagogic hypersynchronies) and during arousal (hypnapompic hypersynchronies)
Delta
• Generally not present in normal adult EEG
• Temporal delta in the elderly it may be acceptable as long as it is <1% of the record.
Normal background for age
|
|
Typical (Hz) |
Limit of normal (Hz) |
|
4 months |
3-4 |
- |
|
5 months |
5 |
- |
|
1 year |
6 |
5 |
|
2 years |
7 |
|
|
3 years |
8 |
6 |
|
6 years |
9 |
7 |
|
8 years |
|
8 |
|
13 years |
10 |
|
|
|
|
|
• “Rules”
o Rule of 3’s and 8’s - 3Hz by 3 months, 6Hz by 1year, 8Hz by 3years, 9Hz by 8 years
o 8 by 8 – 8Hz by 8years
Amplitude
• Measured peak to peak
• Low 0-25uv
• Moderate 25-75uV
• High >75uV
Reactivity
• Change in EEG activity due to sensory stimulus or sudden change in internal state
Includes:
• Alpha attenuation with eye opening
• Slowing with hyperventilation
• Cessation of Mu with moving contralateral upper limb
• Response to painful stimulus
• Photic driving response
Sleep
|
Drowsiness |
Decreased background voltage Posterior rhythm slows - theta slowing can
be seen (sometimes in runs 4-8Hz) Diffuse increase in fast activity Slow lateral eye movement |
|
Stage I |
Vertex waves |
|
Stage II |
Vertex waves Sleep spindles 11-15Hz K-complexes (usually seen in stage II but
do not define it) |
|
Stage III |
Delta activity >20% of epoch |
|
Stage IV |
Delta activity >50% of epoch |
|
REM |
Resembles stage I with some slower
elements, low voltage background. Rapid eye movements. Theta waves (saw-tooth waves in central
areas) |
K-complex
• Moderate to high amplitude, diffuse/centrally predominant biphasic, slow wave transients
• At least 0.5sec long and are at least 75uv in amplitude.
• Initial phase usually negative
• Can also be triggered by partial arousal – e.g. lightly tapping noise near patient during stage 2 sleep can induce.
• Unknown what the origin of the name “K” is from
Sleep spindles
• Regular, rhythmic, sinusoidal or spindle shaped waves at 12-14Hz
• Low amplitude
• Predominant in frontal or central regions
• Typically 1-3 seconds
Sleep in children
(See below for Neonatal EEG including sleep)
Vertex waves
Spindles
REM sleep
Activating procedures
Eye opening and closing
• To see PDR and determine its reactivity
• May induce epileptiform activity in some childhood epilepsies
Mental Alerting
• Getting the patient to do tasks to ensure they are alert
• Ensures any background slowing is real – rather than due to drowsiness
Hyperventilation
• Usually done for 3-5min
• Induces respiratory alkalosis
• Normal response is
o Slowing of PDR
o Gradually increasing theta, often polymorphic and widespread
o Followed by delta, often high amplitude
o Referred to as – hyperventilation hypersynchrony OR hyperventilation induced, high amplitude rhythmic slowing.
• Initially frontal in adults
• Subsides 60-90sec after HV
• More prominent in younger patients and with low BSL
• Contraindications:
o Chronic hear to lung conditions
o Pregnancy
o Recent stroke or sub-arachnoid haemorrhage
o Sickle cell disease
o Moya-moya
Abnormalities that can be induced:
• Generalised spike and waves discharges
• Focal spikes
• Lateralised slowing
• Normal HV changes have gradual build-up whereas induced spikes will be sudden
• During hyperventilation hypersynchrony children may have reduced responsiveness – so this should be used with caution in interpretation
Photic Stimulation
• Strobe light flashed at 1-35Hz for 5-10sec each frequency
Visual evoked potentials/Photic driving response
• Positive wave seen in occipital region ~100msec after flash
• Photic driving response is train of VEPs
• Flash can often entrain at low frequencies but not at high
• Can sometimes be seen at subharmonic frequency (e.g. 21Hz flash induces 10.5Hz driving response) or harmonic (i.e. twice the frequency
• The ability to produce a driving response at high frequency (H reponse) has been said to be associated with migraine
• Absence of response is not abnormal
• A very high amplitude driving reponse has been associated with some neurodegenerative disorders (e.g. neuronal ceroid lipofuscinosis)
Photomyoclonic response
• Brief repetitive muscle spikes over anterior regions of the head.
• Often increase gradually in amplitude as stimulation continues and cease promptly when the stimulus is withdrawn.
• Frequently associated with eyelid flutter, a vertical oscillation of the eyelids and eyeballs; sometimes it is associated with discrete jerking, mostly involving musculature of the face and head
• Overall <1% of EEG’s
• No association with epilepsy.
• More common in patients who are anxious or have a psychiatric disorder
Photoparoxysmal response
• Generalised spike wave discharges elicited by photic stimulation
• Photoconvulsive response if photic stimulation triggers convulsion
• Most often seen in the generalised epilepsies such as JME, but can be seen in patients with focal epilepsy
• Features that correlate with increased association with epilepsy:
o Frontal predominant
o High voltage discharge
o Spike wave outlasting the photic stimulus
• Waltz et al. classified PPR into four types (of increasing significance):
o Type 1, spikes with occipital rhythm;
o Type 2, parieto-occipital spikes with a biphasic slow wave;
o Type 3, parieto-occipital spikes with a biphasic slow wave and spread to the frontal region;
o Type 4, generalized spikes and waves or polyspikes and waves.
• There are other classification systems
• The presence of a PPR does not necessarily mean the patient with have photosensitive seizures
|
PPR |
Photic induced Sz |
Other seizures |
|
|
Epilepsy with PPR |
Yes |
No |
Yes |
|
Epilepsy with mixed
seizures |
Yes |
Yes |
Yes |
|
Pure photosensitive
epilepsy |
Yes |
Yes |
No |
• With a generalised (type 4) PPR the risk of epilepsy is 70-90%
o Likelihood of visually induced seizures is:
- 60% overall
- 30% if there are no epileptiform discharges, except in PPR
• A PPR can be seen in non-epileptic patients and is more common in relatives of epilepsy patients
• More common in younger patients with epilepsy group:
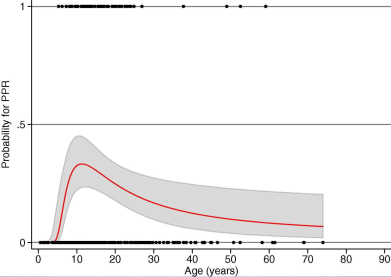
Aurlien et al Clinical Neurophysiology 2009
•
Artifacts
• Electrode ‘pop’
• Muscle
• Chewing/tongue
• Perspiration
• ECG artefact
• Pulse artefact
• Electrical Artifact (50Hz)
• Eye blink
• Eye movements
Normal Variants
Variant |
Morphology |
Location |
State |
Age |
Reactivity |
Age dependent variants |
|||||
|
Posterior slow waves of youth |
Theta and delta (2-4Hz) mixed with the posterior dominant rhythm |
Bilateral, asymmetrical |
? |
Age 7-20 |
|
|
Hyperventilation
induced slowing |
Rhythmic high
amplitude theta/delta |
Generalised –
more posterior in children, anterior in adolescents |
During HV –
should cease within 1 min of HV |
<30 years |
|
|
Temporal theta |
4-5Hz theta |
Temporal leads |
|
Elderly |
Hyperventilation |
Rhythmic variants |
|||||
|
Alpha variant –
slow |
Half frequency
of standard alpha |
Posterior
dominant |
Wake |
|
Attenuate with
eye opening |
|
Alpha variant -
fast |
Twice alpha
frequency, notched or bifurcated |
|
|
|
|
|
Mu |
Arciform 8-11Hz |
Central Uni or Bilateral |
Wake |
Young Decreases with age |
Attenuate with contralateral arm movement |
|
RMTD |
5-7Hz theta Monomorphic, fixed frequency. |
Mid temporal Unilateral, can shift laterality |
Drowsy/light sleep |
Young adults |
|
|
SREDA |
Runs of diffuse, monomorphic theta (5-6Hz) |
Bilateral but can be asymmetrical or more focal |
Wake/ Drowsy/ light sleep |
Adults and elderly |
|
|
Midline theta
rhythms |
5-7Hz, smooth
or arc shaped (mu like) |
Cz and nearby |
Wake/drowsy |
|
|
Epileptiform patterns |
|||||
|
Wicket spikes |
Arciform 90-150ms, <200uV Isolated or in trains |
Mid temporal |
Drowsy/light sleep |
?Any |
|
|
SSS/BETS |
Mono or biphasic spikes Duration <50ms Amplitude >50uV |
Mid temporal, oblique dipole Uni or bilateral Synchronous or asynchronous |
Stage I or II sleep |
?Any |
|
|
PSW/6Hz spike wave |
5-7Hz burst of spike and slow wave Small spikes buried in slow wave Last 1-2 sec |
Bilaterally synchronous |
Drowsiness/light sleep |
Young adults |
WHAM and FOLD varieties |
|
14 and 6Hz positive waves |
0.5-1sec run of positive, arciform sharp waves |
Posterior temporal and occipital |
Drowsiness/light sleep |
Children/young adults |
|
Lamba/POSTS |
|||||
|
Lambda |
Single, positive, sawtooth/ triangular waves 160-250ms |
Occipital Bilateral but asymmetrical |
Wake |
Young Decreases with age |
Promoted by scanning /saccadic eye movements |
|
POSTS |
Similar to lambda, may be biphasic May occur in trains |
Occipital Usually synchronous |
Stage I and II sleep |
Young Decreases with age |
|
|
|
|
|
|
|
|
Alpha variants
• Harmonics of normal alpha
• Fast alpha variant (harmonic) – twice normal alpha frequency
• Slow alpha variant (subharmonic) – 4-5Hz, notched appearance
• Reactive to eye opening, stimulation
• Same features as normal alpha activity
Mu rhythm
• Sharply contoured, arch shaped
• 8-11Hz (tend to occur at similar frequency to patients background)
• Central regions – unilateral or bilateral
• Attenuate with arm movement or thought of movement
• Does not attenuate with eye opening (to differentiate from alpha)
• Disappear with sleep
• Seen in younger individuals and decreases with age
Lambda waves
• Single, occipitally based positive waves, sawtooth
• Usually bilateral, but often significant asymmetry
• Probably a form of visual evoked potentials (increased by visual scanning tasks)
• Occur when eyes open, not seen in sleep
• Seen in younger individuals and decreases with age
Positive Occipital Sharp Transients of Sleep (POSTS)
• Monophasic, triangular waveforms, positive (similar to lambda waves)
• Occipital regions
• Occur in stage I and II of sleep (not in wakefulness)
• Usually synchronous
• May occur in trains of 4 or 5, but not rhythmic
Wicket spikes/ Wicket Rhythms
• Sharp waves 90-150ms duration, <200uV amplitude
• Appear similar to mu – i.e. arciform
• Occur in trains or isolated
• Often when drowsy and light sleep
• Mid-temporal
• Symmetrical (c.f. epileptic discharges)
Rhythmic (Mid)Temporal Theta Bursts of Drowsiness (RMTD)
• Also previously known as Psychomotor variant
• 5-7Hz discharge in the temporal area, occurs in relaxed wakefulness or drowsiness
• Sharp on one side, rounded or flat topped on the other
• Monomorphic, constant frequency, does not evolve
• Can shift laterality
• No after-going slow waves
• Young adults
SREDA (Subclinical Rhythmical EEG Discharges of Adults)
• Bilateral, diffuse discharges, temporal (and parietal) regions, 5-6Hz
• Can be asymmetric or appear more focal
• Usually 20-40sec, but can last minutes
• Relaxed wakefulness or drowsiness
• Occur in adults and elderly
• Monomorphic theta sharp waves
• Compared to true epileptiform discharge:
o No clear cut spikes
o No recruitment
o No alteration in consciousness
o Does not (?rarely) occur in sleep
o No post-ictal slowing
Small Sharp Spikes/ BETS (benign epileptiform transients of sleep)
• Mono or biphasic spikes, amplitude <50uV, duration <50ms
• Sleep stages I and II
• Mid temporal
• Complex polarity, oblique dipole extending over both hemishperes (atypical for epileptifrom discharge)
• Unilateral or bilateral, synchronous or asynchronous
• Some lingering argument as to an association with epilepsy
Phantom Spike-Wave Discharges
• Also called: 6Hz Spike and Waves Bursts OR Six per second spike wave
• 5-7Hz, bilaterally synchronous burst of spike and slow wave
• Spike often low amplitude and buried in slow wave
• 1-2sec bursts
• Seen in drowsiness and light sleep
• Adolescents and young adults
• FOLD – Female, occipital, low amplitude, drowsy - Benign
• WHAM – wake, high amplitude, anterior, male - Some association with epilepsy
14 and 6Hz Positive Spikes
• 0.5-1sec runs of positive sharp waves
• Arciform or comb shaped
• Frequency either ~14Hz (most common) or ~6Hz
• Widespread field, best seen over posterior temporal and occipital areas
• Usually bilateral but asynchronous
• Drowsiness and light sleep, usually up to young adulthood
• Positivity best seen in a referential montage
Lateral Rectus Spikes
• Occur with contraction of the lateral rectus muscles
• Low amplitude, short duration
• Seen best in F7/F8
• Very sharp
• Disappear in non-REM sleep when eyes relaxed
Posterior slow waves of Youth
• Theta or Delta waves that intermix with the posterior rhythm
• From about age 7 to 20
• Occipital areas
• Suppress with eye opening
• Should not exceed PDR amplitude by more than 50%
• Can be asymmetrical
Abnormal EEG
Focal abnormalities
Epileptiform discharges – see epileptiform section below
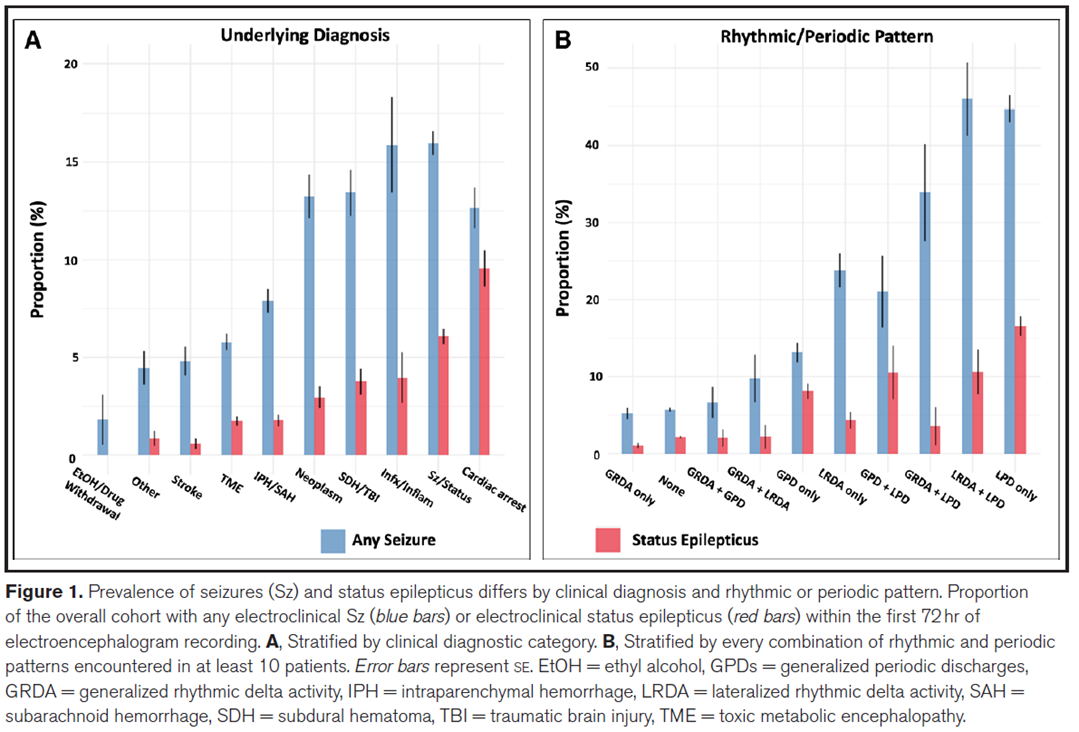
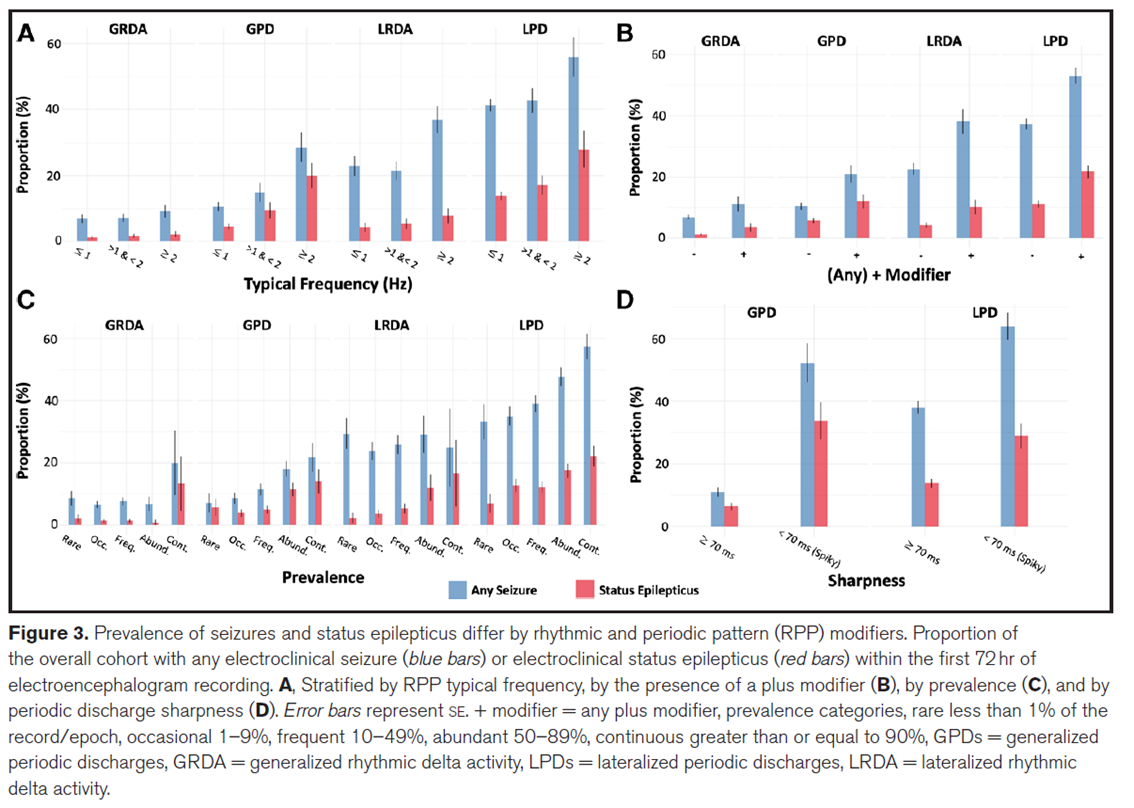
Lateralised Periodic Discharges (LPDs) [Previously Periodic lateralized epileptiform discharges (PLEDS)]
• Periodic – occurring with a interdischarge interval i.e. occurring regularly every second or so.
• Usually broad, high voltage sharply contoured slow wave or sharp and slow wave complex (sometimes more triphasic appearance)
• Indicative of underlying acute pathology
• Associated with
o HSV encephalitis
o Stroke
o Tumour
o Abscess
o
PLEDS Plus +
• PLEDS with admixed faster rhythms/low amplitude polyspike
• Stronger association with epilepsy, 70% will go on to have a seizure
Poly-PLEDS
• Polyphasic/polyspike discharges
• Very high association with seizures
Bilateral independent Periodic Discharges (BIPDs) [Previously BiPLEDS]
• LPDs in both hemispheres that are not occurring synchronously (if synchronous would be GPDs – see below)
• Global or multifocal cerebral insult
Generalised LPDs (GPDs)- discussed below
Unilateral Independent Periodic Discharges (UIPDs)
• Similar to LPDs but where there are more than one periodic discharge (e.g. if you have a left temporal LPD and also a left parietal LPD occurring at a different frequency).
Brief potentially ictal rhythmic discharges (BIRDs)
• Brief (<10 sec) runs of high frequency rhythmic activity
• “Too short” to be a seizure, however highly predive of seizures
Focal Polymorphic Slowing
Focal intermittent Polymorphic Delta activity
• Arrhythmic delta with changing frequency, amplitude and morphology
• Associated with focal structural abnormality affecting the underlying white matter (cortical deafferentation)
• Localising value is increased with the fast beta frequencies are also attenuated in the same region.
Persistent (Continuous) Polymorphic Delta Activity
• Irregular delta activity (as above)
• Delta activity present for >50% of record
• Typically seen in:
o White matter lesions
o Post-ictal states
o Ipsilateral thalamic lesions
Focal monomorphic slowing
Said to more likely represent underlying grey matter dysfunction
N.B. cortical
Intermittent Rhythmic Delta Activity
• Thought to arise from dysfunction of the subcortical centres influencing the cortex
• Similar finding is seen in hyperventilation
o Adults tend to show frontally predominant – like FIRDA
o Children show occipitally predominant – like ORIDA
GRDA (Generalised intermittent rhythmic delta activity) [previously FIRDA (frontal intermittent rhythmic delta activity)]
• Short bursts of, rhythmic, synchronous bifrontal delta activity
• Often high amplitude
• Lasts only a few seconds
• Present in wakefulness and drowsiness, disappears in sleep (may return during REM)
• Non-specific aetiology - some type of cerebral disturbance – focal or diffuse
o E.g. Toxic, metabolic encephalopathy, raised ICP, deep focal lesion
OIRDA (occipital intermittent rhythmic delta activity)
• Typical ORIDA lasts only a few seconds
• Occurs during wakefulness
• In general non-specific aetiology – as per FIRDA
• Association with absence epilepsy
o Present in 15-30% of young patients with absence epilepsy – usually at 3-4Hz
o Correlated with increased sensitivity to hyperventilation
o Unlike ‘typical ORIDA’ can have very long runs
LRDA (Lateralised rhythmic delta activity) [Previously TIRDA (Temporal intermittent rhythmic delta activity)]
• Focal rhythmic delta slowing
• Unlike ORIDA/FIRDA it is a localising abnormality – suggestive of temporal lobe dysfunction/epilepsy
• Strong association with the presence of temporal lobe spikes
• Almost always ipsilateral to epileptiform focus
• Rarely can be ‘false localising’ and associated with extratemporal lobe focus
Generalised abnormalities
Generalised slowing
• Three forms (levels of severity)
o Background slowing
- Rhythm too slow for patients age
o Intermittent slowing
- Bursts of generalized slowing
o Continuous slowing
- Polymorphic delta activity for >80% of tracing
• Graduated from best to worst
• Most commonly associated with encephalopathy (= diffuse cerebral disturbance/dysfunction)
• No specific aetiology
Periodic patterns – GPDs (Generalised periodic discharges) [previously GPEDS]
• Periodic (i.e. regular) bursts of activity
• Complex, epileptiform
• Similar to PLEDs/Poly-PLEDS but generalized, can be called GPEDs
• Some reserve the term GPEDS for when there is no normal background between the discharges
• If there is normal background between the discharges then they may be better described as frequent interictal discharges or status epilepticus
• GPEDS are associated with a poor prognosis in obtunded patient (particularly post anoxic brain injury)
• Aetiology
o Any severe cerebral injury
o A variety of GPEDs/triphasic waves may be seen in CJD
o SSPE – discharges every 3-20seconds
Burst-suppression
• Bursts on quiet background
• Indicative of severe encephalopathy
• Prognostic significance depends on clinical scenario
o May indicate medication effect/overdose – esp. barbiturate – in which case full recovery may be expected
o In setting of post-anoxic injury it is a very poor prognostic marker
Background suppression
•
Electrocerebral inactivity
• Brain death
Triphasic waves
• Triphasic morphology – typically negative, positive, negative
• May have anterior-posterior lag
• Were specifically associated with hepatic encephalopathy but can occur in multiple encephalopathies
• A variety of triphasic waves is seen in CJD
CJD Pattern
• Periodic ~1Hz
• Triphasic waves – however may be sharper, more epileptiform (similar to GPEDs)
• May be more posterior in variant disease
Alpha-pattern coma
• Diffuse alpha pattern
• Occurs after arrest, pontine stroke and some drug overdose
• Had been thought to predict poor prognosis
Spindle Coma
Epileptiform abnormalities
Definition
• Spike
(<80msec)
•
Sharp wave (80-200msec)
•
Spike-wave
IFCN definition
(1) Di- or tri-phasic wave with pointed peak;
(2) different wave duration than the ongoing background
activity;
(3) asymmetry of the waveform;
(4) followed by a slow after-wave;
(5) the background activity is disrupted by the presence of
the IEDs
(6) voltage map with distribution of the negative and positive potentials suggesting a source in the brain corresponding to a radial, oblique, or tangential orientation of the source
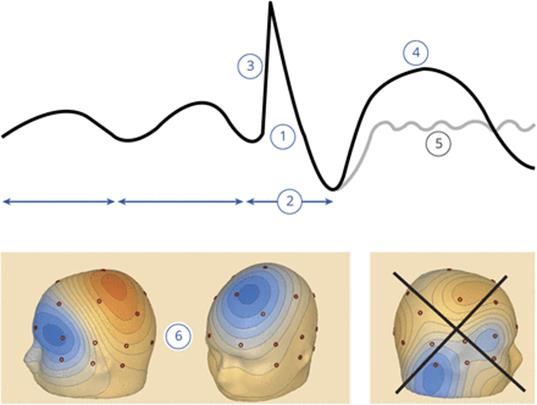
(From Kural MA, Duez L, Sejer Hansen V, et al. Criteria for defining interictal epileptiform discharges in EEG: A clinical validation study. Neurology. 2020;94(20):e2139-e2147. doi:10.1212/WNL.0000000000009439)
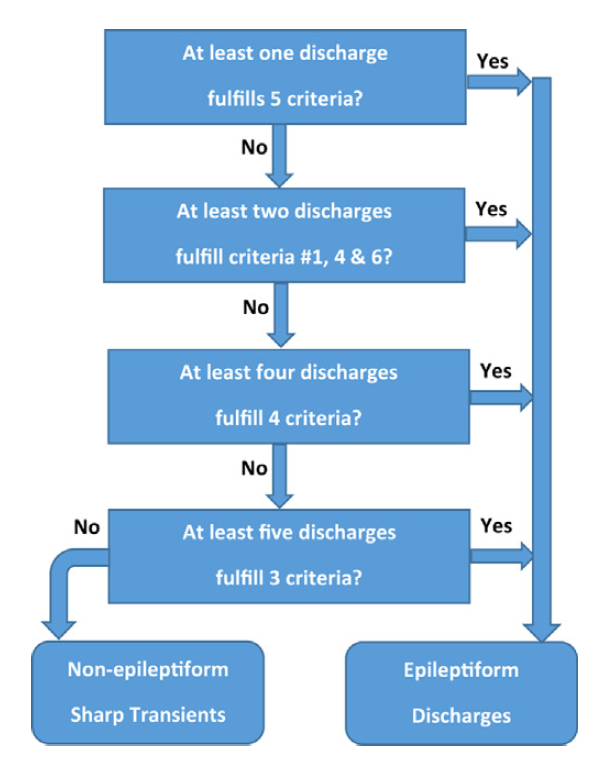
(From: Kural MA, Qerama E, Johnsen B, Fuchs S, Beniczky S. The influence of the abundance and morphology of epileptiform discharges on diagnostic accuracy: How many spikes you need to spot in an EEG. Clin Neurophysiol. 2021;132(7):1543-1549. doi:10.1016/j.clinph.2021.03.045)
Focal
Generalised
Spike wave
• Spike – negative polarity 30-60ms, followed by dome shaped wave of negative polarity 150-200ms
• Analysing aEEG one study found 96% of individual discharges are symmetric but only 24% typical morphology
• Maximal amplitude typically over fronto-central region
• Field maxima during absence seizures Fz, with spread to F3, F4 and Cz.
• Classically discharges are considered regular, although studies suggest 60% are irregular.
• Frequency
o JME - >3.5Hz
o JAE – 3.25 Hz
o CAE – 3Hz
o
Seizures
Tonic-clonic
• Tonic phase
o Spikes and polyspikes
o 10Hz
o Increase in amplitude and decrease in frequency during first 10-20sec
• Clonic phase
o Bursts of generalised high amplitude spike and slow wave or polyspike coninciding with clonic jerks
o Frequency gradually decreases
• Attenuation then diffuse slowing
Absence
• 3Hz spike-wave
o The distinction between an ictal and interictal discharge can be difficult in this situation.
o A seizure might be defined by a change in clinical state or length of discharge (generally considered >2-3sec)
Atypical absence
• Slow spike and wave
• As seen in LGS
Myoclonic
• Polyspike-wave 5-6Hz
Tonic/Atonic
• Paroxysmal fast activity/electrodecrement
Infantile Spasms
• Slow wave followed by electrodecrement
Focal seizures
• Often begin with rhythmic theta
• Evolve - higher amplitude and faster or slower frequency
• Often end abruptly, but can wane
• Can be rhythmic beta (more often seen with intracranial electrode recordings)
• Sometimes rhythmic spikes or sharp waves (similar to the interictal)
Encephalopathies
- Hepatic
encephalopathy
- Diffuse
triphasic waves
- HSV
- PLEDs – 1-4
seconds
- Usually
unilateral – temporal region
- Low
sensitivity, high specificity
- sCJD
- Generalized
periodic sharp wave complexs (PSWC)
- Like PLEDs
but generalized (GPEDs)
- Typical ~1Hz
- Often
triphasic
- Sens 65% but
Spec ~90%
- Do not occur
in vCJD
- SSPE
- Generalized
periodic complexes lasting up to 3 sec with 3-15sec intervals.
Neonatal EEG
• Timing of EEG patterns is described in terms of post-conception age (CA)(i.e time since LNMP)
• Described as CA (i.e. CA 40 is term)
Sleep stages
• Awake
• Active sleep
o Analagous to REM sleep (except unlike adults, baby is not ‘paralysed’)
o Eye closed
o Baby moves and squirms
o Rapid eye movements
o Facial movements/grimacing
• Quiet sleep
o Deep sleep – evolves into slow wave sleep
o No eye movements
Background patterns
• Low Voltage Irregular (LVI)
o Low voltage (15-35uV), mixed frequencies
o Mainly delta and theta
o Wakefullness and active sleep
• Mixed Pattern
o Similar to LVI but with higher voltages and more slow frequencies
• High voltage slow (HVS)
o Continuous, irregular mixed frequencies but higher voltages (50-150uV)
o Delta frequencies more common
• Trace alternans
o Bursts of mixed activity 2-8 seconds
o Flatter interbursts of 4-8sec
o Bursts and interbursts are of similar length
o Pattern evolves with time:
o Interbursts gradually get shorter
o More activity fills in the interbursts
o Interhemispheric synchrony increases
• Trace discontinu
o Very high voltage polymorphic bursts, often containing sharp features/polyspikes
o Separated by flat periods of up to 10-20sec
o Looks like burst suppression
o Normal pattern of early prematurity
Synchrony
• Exists up to 30 weeks then become asynchronous (transition from trace discontinue to alternans)
• Synchrony then increases again as term approaches (transition from trace alternans to HVS)
Continuity
• Should be established in wakefulness by 34 weeks
• In quiet sleep starts to be seen from 38 weeks.
• There should be no discontinuity after 48 weeks
Graphoelements
• Specific wave forms that appear and disappear at certain CA’s
• Delta Brush
• Sharp transients
• Frontal transients
• Temporal sharp transients
• Vertex waves
o Seen from 8 weeks (CA 48)
• Spindles
o Appear at CA 44-46 (i.e. from 2nd month of life)
o Spindles tend to be asynchronous up to age 2
o Spindles are longer in childhood and get shorter
Intensive care/Critical Care EEG
• Predictive patterns