• Indication for treatment
o Functionally disabling symptoms
o Objective evidence of neurological impairment
•
o Mild sensory attacks often not treated
• Treat infection if it is trigger
• Steroids
o Methylprednisolone 500-1000mg daily
• +/- short prednisolone taper
• Chance of worsening at 5 weeks is reduced (OR 0.37, ARR 25%)
• No difference in outcomes at one year.
• Plasma exchange
• Has been shown to be beneficial in severe or refractory cases.
Interferon beta
Efficacy
• 18-34% reduction in annualised relapse rate
•
Betaferon - Initial
placebo controlled trial - Neurology. 1993;43(4):655
• INCOMIN trial – Avonex vs betaferon – favoured latter. Another Danish study found similar efficacy.
• PRISIMS trial (Rebif vs placebo)
• EVIDENCE trial (Neurology. 2002;59(10):1496) Rebif vs AVONEX – favoured Rebif
• In general terms the evidence for Avonex suggests it may be less effective on some parameters of treatment.
Adverse effects
Contraindications:
• Hypersensitivity to interferon
Adverse effects:
• Injection site reaction – 50% (reduce slightly over time)
• Influenza like symptoms – 40% (reduce to 25% over time)
• Myalgia/arthralgia
• The risk of depression has been raised – however appears similar to placebo group
Complications:
• Increased LFTs – occurs in up to 37%, severe in 1-2% - usually transient
• Decreased white cell count in ~7%
• Severe or symptomatic decreases in white cell count or platelet count have occurred very rarely
• Thrombotic microangiopathy has been noted rarely in case reports
• Seizures have noted in rare case reports
Pregnancy and breastfeeding
• No increase in major congenital malformations
• Safe with breastfeeding
Dosing
• Interferon beta – 1b (Betaferon) 0.25mg SC second daily
• Interferon beta – 1a
o Avonex - 30mcg IM weekly
o Plegridy (Pegelated) – SC every 2 weeks
- Titration – 1st dose 63mcg, 2nd dose 94mcg, ongoing dose 125mcg
• Interferon beta – 1a (Rebif) 22 or 44mcg SC three times/wk
Monitoring
• FBC/LFT ~ 6 weeks after starting and 6 monthly thereafter
Glatiramer
(Copaxone)
• Mixture of random polymers from 4 amino acids
• Antigenically similar to myelin basic protein, distracts immune cells from destruction of myelin sheath
Efficacy
• Lowers relapse rate ~25% (1.19 vs 1.68), reduction in T2 lesions
• No evidence of preventing progression of disability
• Similar efficacy to IFN, similar tolerability, different SE profile (see BEYOND trial below)
Adverse effects
• Injection site reactions (22%)
o Redness, pain, pruritus, mass
• Lipoatrophy
• Immediate post injection reaction (2%)
o Transient chest pain, flushing, dyspnoea, palpitations/anxiety, constriction of the throat, urticaria.
o Can occur with any injection, random
• Lipoatrophy (0.5%)
• Skin necrosis (case reports only)
Pregnancy and breastfeeding
• No increase in major congenital malformations
• Safe in breastfeeding
Dosing
• 40mg SC 3x/week
Monitoring
• FBC/LFT 6 weeks after starting and yearly thereafter
Fingolimod (Gilenya)
Mechanism
• Analogue of Sphingosine 1-phosphate (S1P)
• Acts as a functional antagonist at S1P receptors
• S1P1 receptors are involved in trafficking of lymphocytes through lymph nodes – fingolimod prevents lymphocyte egress from lymph nodes.
• Fingolimod is non-specific and also bind to S1P 3, 4 and 5 receptors.
Efficacy - Trials
TRANSFORMS – NEJM 2010 362:402
• Fingolimod 1.25mg vs 0.5mg vs Interferon beta 1a (avonex) 30mcg
• Primary end point – Annual relapse rate
o 0.2 vs 0.16 vs 0.33
• Progression of sustained (>3months) disability
o Hardly any patients had progression of disability – no difference between any groups
FREEDOMS trial – NEJM 2010 362:387
• Fingolimod 1.25mg vs 0.5mg vs placebo
• Annualised relapse rate - 0.18 vs 0.18 vs 0.4
• Absence of disability progression at 2 years – 83.4 vs 82.3 vs 75.9 (significant)
Adverse effects and Contraindications
Contraindications
• Bradycardia or conduction abnormalities
• Other unstable heart disease
• Active or latent infections (including HBV, HCV, HIV)
• Severe liver dysfunction
• Lymphopenia
• Macula oedema
o ?previous uveitis
Adverse effects
• Muscle/back ache -
rare
• GIT – diarrhoea,
nausea – very rare
Complications
• Bradycardia
o
Only with first dose (or if after prolonged break
from medication)
o
Contraindicated in patients with heart block
o
Caution if on negatively chronotropic drugs
• Increased liver
function tests
o
Increased ALT ~7%
- Cease
treatment if >5x ULN, most LFTs return to normal despite continuing
treatment.
• Lymphopaenia
o Average lymphocyte count falls 75% (from 1.8 to ~?0.5)
o No increased risk of infection has been demonstrated with this fall – lymphocytes are still present, just not in circulation.
o Concern that very low count (<0.2) could result in increased infection risk
• Infections
o
Herpes virus infection
- Increased risk of
VZV infection and HSV
- Rare cases of
disseminated VZV and fulminant HSV encephalitis
• PRES – rare cases
reported ?association.
• Hypertension –
increase of 3mmHg over placebo
• Macular oedema
o
1/300 risk
o
Majority of cases within first 6 months
o
Majority of cases reversible
o
Biggest risk factor is previous uveitis. Uncontrolled DM also a risk factor.
• Excess skin cancer
risk
• PML
o Update report of Novartis database 2018 (Neurology 2018;90, pg 920)
o Risk of PML in patients treated with Fingolimod 0.069/1000pts
o Incidence 3.12/100,000 patient-years
o Not associated with lymphopaenia
o 14/15 pts had been treated for >2 years
Pregnancy and breastfeeding
• Some cases of congenital malformation - ?unclear if above background risk
o Advise patients to avoid in pregnancy
• Breast feeding – transferred in breast milk – breast feeding not advised.
Pharmacology and Interactions
• Half life 6-9 days – steady state after ~1 months
• Complete elimination from the body ~2 months
• Caution with any negatively chronotrophic agents that may exacerbate bradycardia
• Ketaconazole can increase fingolimod levels
• Carbamazepine and other strong CYP450 inducers may result in reduced fingolimod levels
Dosing
• 0.5mg BD for all
• No need to dose adjust for renal or hepatic impairment
Pre-treatment screening
|
Test |
Reason |
|
BHCG
or urine pregnancy test |
Increased
risk of foetal malformation |
|
FBC |
Lymphopenia often occurs |
|
LFT |
Raised
LFTs can occur |
|
Hepatitis B and C |
Risk unknown, excluded from trials. |
|
VZV
IgG |
Disseminated
zoster has occurred. Vaccinate if
negative. |
|
HIV |
Risk unknown, excluded from trials. |
|
Quantiferon gold |
No
known increased risk. |
|
CXR (optional) |
Any evidence of TB or other infectious disease. Baseline. |
|
ECG |
Bradycardia
or heart block – worsened by fingolimod. |
|
Skin Check |
Possible increased risk of skin cancer. |
|
Ophthalmology
review or macula OCT |
Baseline
for macula oedema. |
|
Respiratory function tests (optional) |
Optional, there may be slight decrease in lung function. |
• Vaccinations
should be completed 6 weeks prior to treatment.
Influenza vaccine can be given while patient is on medication, however
may not be as effective.
Advice to patients
• Drug must be taken continuously – breaks in treatment may lead to bradycardia on restarting
• Watch for:
o Rash (particularly shingles)
o Jaundice
o Visual distortion (consider screening with Amsler grid)
• Vaccinations:
o Try and get vaccinations done prior to treatment
o Annual influenza vaccine encouraged
o Avoid live attenuated vaccines while on treatment
• Women – avoid pregnancy, ensure adequate contraception, notify treating team immediately if pregnant
Teriflunomide (Aubagio, Teriflagio)
Mechanism
• Inhibits pyrimidine synthesis
Efficacy - Trials
• TEMSO trial
o 7mg or 14mg Vs Placebo (all figures below are for the 14mg dose)
o RRR ~31%
o Annual Relapse Rate from 0.5 vs 0.37
o Decrease in EDSS progression at early time points
o MRI T2 lesion accumulation over 2 years - ~64% relative reduction
• TOWER
o Teriflunomide 7mg vs 14mg vs Placebo (Results for 14mg below)
o 1169 patients
o RRR 36% (0.5 vs 0.32)
o Time to sustained disability progression – (15 vs 21%) reduced HR 0.65
o The Lancet Jan 2014
• TENERE trial
o Teriflunomide 7mg or 14mg vs IFNB-1a (Rebif) (results for 14mg shown below)
o 324 patients
o Primary outcome was “Treatment failure” (either a relapse or discontinuation) – there was no significant difference.
- With teriflunomide – less patients discontinued, however more patients relapsed
- Drop out 13.5% vs 24% (i.e. if you could stay on IFN would probably be better off?)
o Relapse rate (after adjustment for dropout) was 0.22 IFN vs 0.26 Teriflunomide
• IFN-B combined with teriflunomide vs IFN
o No major safety concerns
o Seemed to be additive effect
o Published in neurology (Freedman 2012)
Adverse events
Contraindications
• Pregnancy
• Liver dysfunction
Serious adverse effects
• Hepatotoxicity
o
Mild elevations are common (although less common
than IFN)
o
Severe elevations occurred in ~2% and this was
similar with placebo and IFN
o
?Cease if >3xULN
• Cytopaenia’s
o
Neutrophils – a minor drop is common (e.g 17% to <1.5 in TOWER, average drop in TEMSO was~1.0),
however severe neutropaenia only occurred in 2
patients in all trials <1%.
o
Lymphocytes – a minor drop is common (avg. drop
0.3), severe lyphopaenia was not observes
Potential adverse effects:
• Respiratory
disease
o
Has not occurred with Teriflunomide but has
occurred in Lefunomide (in patients with RA on
methotrexate)
• Peripheral
neuropathy/paraesthesia
• Serious
Infections – there was no significant difference
• Nasopharyngitis
– overall there was no significant increase across the trials
Less serious side effects
• Diarrhoea (TEMSO -Placebo vs drug; 9vs18%)
• Nausea
(7% vs 14%)
• Hair
thinning (3% vs 13%) (reversible)
Pregnancy
• Category
X
• Has
caused defects in animals
• Is
excreted in semen and therefore should not be used by men wishing to farther a
child.
• Not
safe with breastfeeding
Treatment of toxicity
• Teriflunomide
has a long half-life which is contributed to by enterohepatic cycling – can
require 3months to clear
• Administer
cholestyramine, 8g every 8 hours, to help wash out
Pharmacology and interactions
• Long half life ~19 days – takes 3 months to achieve steady state
• Takes average 8 months for drug to washout to a level safe for pregnancy.
• Minimal significant drug interactions
Dosing
• 14mg tablet daily
Pre-treatment screening
• MRI
brain
• FBC,
Electrolytes, LFT
• HBV
serology
• HCV
serology
• Varicella
IgG
• HIV
• Quantiferon
• Pregnancy
test
Ensure all appropriate vaccinations have been given
Monitoring
• FBC and LFTs every month for 6 months then every 2 months ongoing.
Dimethyl Fumarate
Mechanism
• Alters cellular transcription - NFkB inhibitor, via Nrf2 stimulation
• Alters pathways involved in immune system homeostasis
• Exact mechanisms not known
Efficacy -Trials
• DEFINE
o 240 Tds vs 240 bd vs Placebo
o RRR ~50% (annual relapse rate) at 2 years
o EDSS progression reduction from 60 weeks
o MRI T2 ~85% reduction
• CONFIRM study
o Annualised RR reduction BG12 vs Glatiramer - 44% vs 29%
Adverse effects
• Flushing (5% vs 38%)
• GI symptoms ~20%
o Nausea, upper abdominal pain, diarrhoea
• The above side effects tend to decrease over the first couple of months to a rate of ~5%
• Reduced lymphocyte count ~5% of patients had count <0.5
• Minor increases in LFTs
Pharmacology and
interactions
• Short half life ~1 hour
• Elimination
~60% via exhalation
Dosing
• 120mg bd as titration for 1-2 weeks
• 240mg
bd ongoing
Pre-treatment screening
• MRI
brain
• FBC,
Electrolytes, LFT
• HBV
serology
• HCV
serology
• Varicella
IgG
• HIV
• Quantiferon
• Consider pregnancy test
• Ensure
all appropriate vaccinations have been given
Monitoring
• FBC and LFTs 6 weeks after treatment and then every 6 months
• Consider pausing treatment if lymphocyte consistently below 0.5
Advice to patients
• Consider taking an aspirin with dose if side effects are problematic
• Vaccinations:
o
Try and get vaccinations done prior to treatment
o
Annual influenza vaccine encouraged
o
Avoid live attenuated vaccines while on
treatment
• Women
considering pregnancy should discuss with treating team first.
Natalizumab
Mechanism
• Antibody against alpha-4 integrins – cell membrane proteins on leukocytes
• Alpha 4 integrin binds to endothelial VCAM-1 allowing ingress into the CNS
• Natalizumab thus Inhibits T and B cell entry into CNS
Efficacy - Trials
AFFIRM
• Natalizumab vs Placebo
• Annualised relapse rate 0.23 vs 0.73 as monotherapy, RRR 68%, ARR 50%
• New MRI T2 lesions at one year – 1.2 vs 6.1
• Disability progression 17% vs 29% at 2 years, RRR 42%, ARR 12%
SENTINEL study (NEJM 2006)
• Enrolled patients who had relapses despite being on interferon-Beta 1a (Avonex)
• Natalizumab vs continued use of Avonex
• ARRate 0.34 vs 0.75 (ARR 41%)
• 2 year cumulative sustained disability progression – 23 vs 29% (ARR 6%)
TOP (registry study)
Adverse effects and contraindications
• Infusion reactions – headache, nausea, dizziness, itch rash etc. (24% vs 18% in placebo)
o <1% chance of serious infusion reaction/hypersensitivity
• Possible small increased risk of other infections
• Pregnancy
o No observed increase in risk of congenital malformations
o Possible alteration in foetal blood counts – particularly if used in late pregnancy
• Breast feeding – likely to be safe in most instances, caution with premature infants.
• Risk of PML (Progressive multifocal leukoencephalopathy) – see below
PML risk stratification
• Latest data from:
Ho PR, et al. I. Risk of natalizumab-associated progressive multifocal leukoencephalopathy in patients with multiple sclerosis: a retrospective analysis of data from four clinical studies.
Lancet Neurol. 2017 Nov;16(11):925-933
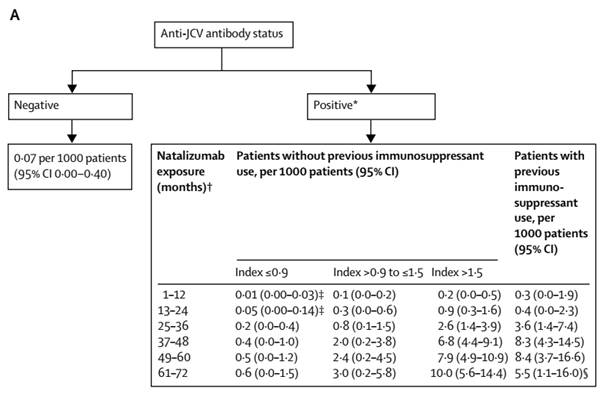
From table above – chance of PML is 1 in……
|
Time |
Index
<0.9 |
>0.9-<1.5 |
>1.5 |
Prior
immune. |
|
1-12
months |
100,000 |
10,000 |
5000 |
3333 |
|
13-24
months |
20,000 |
3333 |
1111 |
2500 |
|
25-36
months |
5000 |
1250 |
385 |
278 |
|
37-14
months |
2500 |
500 |
147 |
120 |
Pharmacology and Interactions
• Antibody with half life ~26 days
• 6% of patients develop neutralizing antibodies
Dosing
• 300mg IV every 4 weeks
Pre-treatment screening
• MRI brain (ideally with gadolinium)
• FBC, Electrolytes, LFT
• HBV serology
• HCV serology
• Varicella IgG
• HIV
• Quantiferon
• Pregnancy test or discussion
• Ensure all appropriate vaccinations have been given
Monitoring
• FBC/LFT 6 weeks after first dose, then every 6 months
o Altered blood count is common – increased lymphocytes, monocytes, eosinophils and basophils with occasional nucleated erythrocytes.
Other issues
· Rebound increase in relapse rate can occur from ~2months – consider starting an alternative therapy early to help prevent this issue.
· Presence of a relapse during the ‘gap’ has been found to be risk factor for ongoing relapse (once starting fingolimod) (Neurology 82 1204-1211 (2014))
· If breakthrough disease occurs on natalizumab – consider testing neutralising antibodies
Advice to patients
• Vaccinations:
o Try and get vaccinations done prior to treatment
o Annual influenza vaccine encouraged
o Avoid live attenuated vaccines while on treatment
• Women considering pregnancy should discuss with treating team first.
• If abnormal blood count is detected this may be an effect of the natalizumab and should be discussed with treating team.
Alemtuzumab
• Anti-CD52 monoclonal antibody
• Depletes lymphocytes
o Lowest levels reached at 1 month point
o After treatment B-cells recover in 7 months, CD8 cells in 20months and CD4 in 35months.
• “After lymphocyte depletion, a distinctive pattern of T- and B- lymphocyte repopulation occurs over time, changing the balance of the immune system”
•
Safety
• Infusion associated reactions
o Cytokine release and due to lymphocyte death and nitric oxide release
o Can cause transient worsening of pre-existing symptoms – conduction block
o Reduce as time goes by
o Pre-treatment with methylprednisolone (probably best to give for each of the 5 days of infusion)/NSAIDs/Anti-histamine
• Autoimmune thyroid disease
o ~ 30%
o Peak at 3 years
• ITP
o 1.7%
o First case died as was unrecognised
o
• Nephropathy
o 7 cases (by 7/2015)
o Anti-GBM
o Membranous Golmerulonerphritis
o 2 early cases required renal transplant – not identified early
• Infection
o Increased rate of mild to moderate infections (77% vs 66% in IFN group)
o Herpes zoster ~0.2-0.3%/year
- Give oral prophylaxis
o Pneumonia
o TB
o Slight reduction as time goes by
• Bradycardia
o Has been identified in follow-up studies
o Never been symptomatic
• Cancer
o No overall increased risk of cancer
o Increased risk BCC - slight
o Increased thyroid cancers – probably because of increased surveillance
Vaccination
• Able to mount good immune response when challenged – therefore vacccinations can still be given
Pregnancy
· See below
Trials
• Initial small trial in patients with advanced disease (largely secondary progressive)
o Negative
Major Phase 2/3 trials
· All vs Rebif (IFN-1a S/C)
|
|
CAMMS223 |
CAMMS223
-extension |
CARE-MS
I |
CARE-MS
II |
||||
|
|
3
years |
5
years |
2
years |
2
years |
||||
|
|
Active RRMS (2relapses in 2 yrs,
at least 1 Gad+ lesion), Rx naïve, EDSS </= 3, Onset </=3yrs |
Active RRMS (2relapses in prior 2 yrs, 1 relapse in last yr), Rx naïve, EDSS </=3, Onset </=
5yrs |
Active RRMS (same as CARE-MSI), relapsing on prior DMT, EDSS </=
5, Onset </= 10yrs |
|||||
|
Rx (Patient
numbers) |
IFN
(111) |
AL
(112) |
IFN (111) |
AL (112) |
IFN (187) |
AL (376) |
IFN (202) |
AL
(426) |
|
ARR |
0.36 |
0.11 |
0.35 |
0.12 |
0.39 |
0.18 |
0.52 |
0.26 |
|
ARR
% reduction |
|
69 |
|
66 |
|
55 |
|
49 |
|
ARR
% absolute |
|
25 |
|
23 |
|
21 |
|
26 |
|
Relapse
free % |
52 |
77 |
41 |
68 |
|
(NS) |
|
42 |
|
SAD% |
24 |
8 |
30 |
13 |
11 |
8 |
21 |
13 |
|
SAD
RRR% |
|
67 |
|
57 |
|
30
(NS) |
|
42 |
|
EDSS
score change |
+0.46 |
-0.32 |
+0.46 |
-0.15 |
NS |
NS |
+0.24 |
-0.17 |
|
MSFC
change |
- |
- |
- |
- |
+0.03 |
+0.11 |
-0.04 |
+0.08 |
|
SRD% |
- |
- |
- |
- |
25 |
23 |
13 |
29 |
|
|
|
|
|
|
|
|
|
|
|
New
or enlarging T2 lesions % |
|
|
|
|
58 |
49 |
68 |
46 |
|
T2
lesion volume median change % |
|
|
|
|
-6.5 |
-9.3 |
-1.2 |
-1.3 |
|
Median
change in brain parenchyma% |
|
|
|
|
-1.5 |
-0.9 |
-0.8 |
-0.6 |
|
|
|
|
|
|
|
|
|
|
|
MRI
and clinically disease free % |
|
|
|
|
27 |
39 |
14 |
32 |
|
Hospitalisation
reduction |
|
|
|
|
|
29
(NS) |
|
55 |
|
|
|
|
|
|
|
|
|
|
SAD = sustained accumulation of disability, SRD = sustained reduction in disability
Active RRMS = >/= relapses in the prior 2 years
Dosing and Monitoring
• Switching from fingolimod 6-8 weeks (Dr Compston opinion)
• Switching from natalizumab ~6 weeks
• Levels of drug in blood low or undetectable within one month
Pre-initiation
|
VZV
serology |
VZV
neg - Vaccinate prior to Rx |
|
HBV,
HCV, HIV serology |
|
|
Quantiferon (TB test) |
|
|
HPV
screening (Pap smear) |
|
|
FBC |
|
|
Electrolytes |
|
|
Urinalysis
with microscopy |
|
|
TFTs |
|
• Complete vaccinations 6 weeks prior to dose, consider:
o VZV
o HBV/HAV
• Women – should use effective contraception during infusion and for 4 months post treatment
Infusion
· Start anti-pyretics and antihistamines starting 1 day prior and running to
On-going monitoring
• Monitoring required for 48 months post last infusion
|
|
Watch for: |
|
|
FBC |
|
Monthly |
|
Creatinine |
|
|
|
Monthly urinalysis and
microscopy |
|
|
|
Thyroid function (TSH) |
|
Every 3 months |
|
HPV screening |
|
Yearly |
|
|
|
|
· Absolute lymphocyte counts do NOT predict response to treatment
Patient advice:
· Women should delay becoming pregnant until 4 months after treatment and are advised to discuss ongoing treatment plan with neurologist prior to conception.
|
(ITP)
Idiopathic Thrombocytopaenic Purpura |
Watch
For: |
Monitoring: |
|
• This is an autoimmune condition that results in a
drop in the number of platelets in the blood • Platelets are one of the components of the blood
which allow it to clot properly • Low platelets can cause bleeding |
• Bruising more easily • Bleeding from a cut that is hard to stop • Menstrual periods that are heavier, longer or more
frequent than usual • Bleeding from your gums or nose • Small scattered spots on your skin that are red,
pink or purple • Blood in your urine, stool or vomit • Coughing up blood |
Monthly
measurement of your platelet count must be done (this is part of a “Full
blood count or FBC) |
|
Nephropathies
(Kidney Disease) |
|
|
|
Antibodies
can attack the kidney and cause it to dysfunction |
• Blood in your urine |
Monthly
testing of kidney function from a blood test Monthly
testing of protein and blood in urine |
|
Thyroid
disorders |
|
|
|
Can
be either • High thyroid function • Low thyroid function |
|
Every
3 months your thyroid function should be tested on a blood test. |
|
Infection |
|
|
|
Because
of its effect on your immune cells some infections are more common and severe |
Fever Chils Muscle
aches Cough Oral
or vaginal thrush Rash Cold
sores |
Testing
can be done depending on your symptoms |
|
|
|
|
Ocrelizumab
Mechanism
• Recombinant, humanised anti-CD20 monoclonal antibody (IgG1 subtype)
• Depletes CD20 B cells
Efficacy - Trials
OPERA trials
• Two trials OPERA I and II published together in one paper (NEJM 2017)
• Total of 1656 patients recruited from 2011-2013
• Compared to Rebif
• Followed for ~2 years
Results
• Very similar for both groups
• Annualised relapse rate 0.16 vs 0.29
o Relative risk reduction 46%
o Absolute risk reduction 0.14
o NNT 7
• MRI new T2 lesions
o 0.32 vs 1.41 and 0.33 vs 1.9 (OPERA I and II)
o Relative risk reduction - 77% and 83% lower
• Disability
o Disability progression 9.1% vs 13.6% (P<0.001)
o Relative risk reduction 40%
o Absolute risk reduction 4.5% (NNT 22) (Over 2 years)
• Side effects
o Infusion reactions ~30%
o No clear signal in increased in infections
Adverse effects
• Infusion reactions (pruritus, rash, throat irritation, dyspnoea, pharyngeal or laryngeal oedema, flushing, hypotension, pyrexia, fatigue, headache, dizziness, nausea and tachycardia)
o 27% with first infucion
o <10% by dose 4
• Infection
o In the trials URTI was the only consistently increased infection (~15% vs 10% - risk 5% or 1/20)
o Possible trend towards increase of other infections (including VZV)
• Possible risks based on long term use of rituximab:
o PML
o Hypogammaglobulinaemia
o Rare, severe sinopulmonary infections.
• Pregnancy – No data. Advise avoid for 6 months after last infusion.
• Breast feeding – unknown, very unlikely that any would cross from ~1 month after infusion.
Pharmacology and interactions
• It is a monoclonal antibody with a half life of ~26 days
• CD 20 cells depleted by 14 days
• 90% return to baseline by 2.5 yrs
• Renal or hepatic impairment are not expected to significantly alter its metabolism
Screening prior to treatment
• Baseline MRI
• FBC
• Electrolytes
• LFT
• Screen for infections
o TB (Quantiferon +/- CXR)
o HBV
(Including HBsAg, Anti-HBc, Anti-Hbs)
o HCV
o HIV
o VZV (vaccinate if not immune)
• Consider pregnancy test
• Consider skin check and other cancer screening if patient is at an increased risk
• Vaccinations should be completed 6 weeks prior to treatment. Influenza vaccine can be given while patient is on medication, but may not be as effective.
Dosing
• 300mg IV Infusion on day 1 and 15 and then single, 600mg infusion every 6 months
• Premedication:
o Methylprednisolone 100mg IV 30 min prior
o Anti-histamine (e.g. loratadine 10mg) 30-60min prior
o Consider paracetamol 30-60min prior
• It is likely that B-cell populations regenerate at different rates in different individuals. B-cell subset levels may indicate this, however have not be studied for ocrelizumab.
Monitoring
• Routine FBC and electrolytes ~6 weeks after initial treatment then prior to next dose
Advice for patients
o Try and get vaccinations done prior to treatment
o Annual influenza vaccine encouraged
o Avoid live attenuated vaccines while on treatment
• Ensure cancer screening is completed as per general population guidelines, annual skin check
• Ensure early investigation and treatment of respiratory or other infections. See your doctor if recurrent infections.
• Women – ensure adequate contraception for 6 months after last dose.
Daclizumab (Zinbryta) - DISCONTINUED
** Discontinued due to cases of hepatic failure **
• Anti-high affinity IL2 receptor antibody
• Initially thought to reduce T cells
• ?more effect on NK cells and other lymphoid activator cells.
Trials
DECIDE Trial
• NEJM 2015
• Daclizumab vs Interferon Beta 1-a (Avonex)
• Recruited 2010-2012
• 1841 patients
• Follow-up median 2 years
Results
• ARR 0.22 vs 0.39
o Relative risk reduction - 45%
o Absolute risk reduction - 0.17 relapses/year
o NNT (For one year to prevent a relapse) = 5.9
• MRI new T2 lesions
o 9.4 vs 4.3
o Relative reduction of 54%
• No significant difference in disability
Adverse events
• Elevation in LFTs >5xULN:
o 6% vs 3% (Absolute diffference 3% - NNH 33)
• Skin reactions
o 37% vs 19% (Absolute difference 18% - NNH 5.6)
o Caused discontinuation in 5% (vs 1%)
o Rash and eczema main problems
o Serious cutaneous events 2% vs 1%
Mitoxantrone
·
DNA topoisomerase inhibitor
·
Effective for both RR and progressive
·
Significant toxicity and SE
· No longer used due to risk of secondary leukaemia
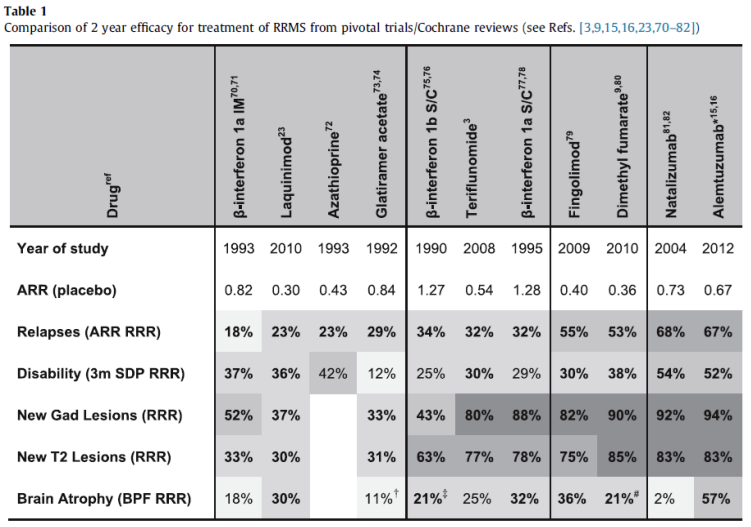
COMPARISONS and other Trials
|
|
TRANSFORMS |
|
SENTINEL |
|
CARE MS II |
|
|
|
IFN-1a IM |
Fingolimod |
IFN-1a IM |
NLZMAB+IFN |
INF-1a S/C |
ALM |
|
ARR |
0.33 |
0.16 |
0.75 |
0.34 |
0.52 |
0.26 |
|
ARR Red% |
|
52 |
|
55 |
|
49 |
|
Absolute Red % |
|
17 |
|
41 |
|
26 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FREEDOMS |
|
AFFIRM |
|
|
|
|
Placebo |
Fingolimod |
Placebo |
NLZMAB |
|
|
ARR |
0.4 |
0.18 |
0.73 |
0.23 |
|
|
ARR
Red% |
|
55 |
|
68 |
|
|
Absolute
Red % |
|
22 |
|
50 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|

Rebif vs Copaxone
REGARD Trial (Lancet Neurology 2008)
Followed for ~2 years – no significant difference in safety or efficacy
Fingolimod vs Avonex
TRANSFORMS – NEJM 2010 362:402
• Fingolimod 1.25mg vs 0.5mg vs Interferon beta 1a (avonex) 30mcg
• Primary end point – Annual relapse rate
o 0.2 vs 0.16 vs 0.33
• New T2 lesions
o Significantly reduced
• Progression of sustained (>3months) disability
o Hardly any patients had progression of disability – no difference b/n any groups
Dimethyl Fumarate Vs Copaxone
• CONFIRM study
o ARRR BG12 vs Glaterimer - 44% vs 29%
BEYOND
• Lancet neurology Oct 2009
• Compared 3 groups - IFN 250ug, IFN 500ug and Glatiramer 20mg – all every second day
• No difference in efficacy between 3 groups
• Similar number had SE but different SE
• Ghjghj
o Ghjghj
• Ghjghjg
Pregnancy and Breastfeeding
Pregnancy
• 20-30%of women diagnosed with MS will have a child after the diagnosis
Effect of MS on pregnancy
• No effect on ability to conceive
• No increase in foetal abnormalities or obstetric complication (some reports have suggested some increased complications but have not been substantiated)
• Should not influence method of delivery or anaesthesia used
Genetic Risk to Child
• Risk in general population is 0.13%, risk if parent has MS is 2-2.5%
• Risk is higher for infants born in ‘spring’ (peak November) and lowest for ‘autumn’ (peak April).
Effect of pregnancy on MS
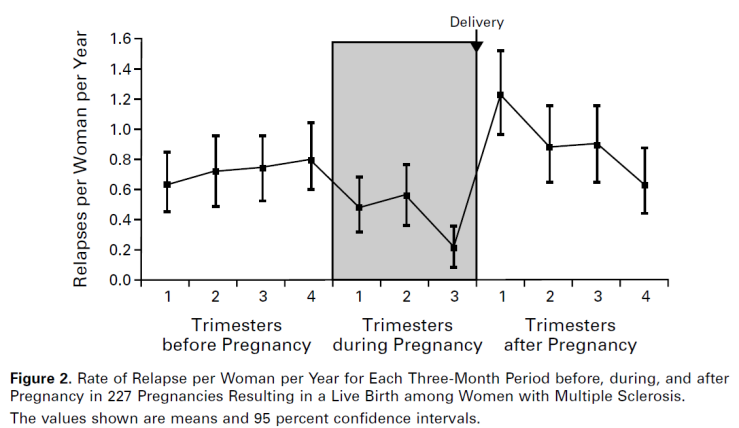
• PRIMS study
• Relapse rates fall by 70% in third trimester
• Relapse rates rebound during the first 3 months post-partum to 70% above prepregnancy level
o Risk factors include – high prepregnancy relapse rate, relapse during pregnancy and higher disability level prior to pregnancy
• Some studies have suggested that more pregnancies is linked to better long term prognosis in RRMS (this was not the case in PPMS)
• Method of delivery and type of anaesthetic did not affect relapse rate (in Italian study on this question)
|
Month |
Relapse
rate |
|
12 months pre-pregnancy |
0.7 |
|
First trimester |
0.5 |
|
Second trimester |
0.6 |
|
Third trimester |
0.2 |
|
First 3 months post-partum |
1.2 |
|
Second 3 months |
0.9 |
|
Third 3 months |
0.9 |
|
Forth 3 months |
0.6 |
NEJM 1998 – PRIMS study
NEJM 1998 – PRIMS study
Effect of multiple pregnancies MS in long term
|
Group |
Median
time to EDSS 6 (years) (of
those who reached this EDSS) |
Estimated
median time to EDSS 6 (years) - (for whole group) |
Estimated
difference relative to group one (years) |
|
Never had children |
8 |
15 |
|
|
Children prior to MS |
10 |
13 |
No
significant difference |
|
Children after diagnosis of MS |
21 |
23 |
8 |
|
Children before and after MS |
21 |
22 |
7 |
|
|
|
|
|
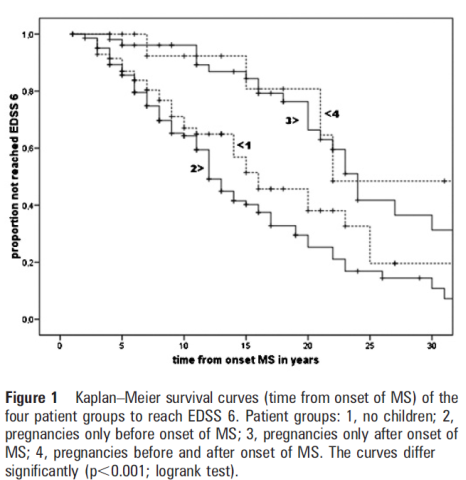
JNNP 2010 81:38
Breastfeeding
• No clear evidence that breastfeeding affects relapse rate
o Multiple studies have shown opposing effects
o A meta-analysis suggested an overall slight benefit of breast feeding
o Further analysis suggested that only exclusive breast feeding for at least 2 months was required to show a benefit
o Another study (Hellwig et al. 2012) also concluded exclusive breastfeeding decreased relapse rate vs non-exclusive or no breastfeeding (0.68vs1.5vs1.68).
o (Hellwig et al 2015 JAMA Neurol) – 201 women, 60% exclusively breastfed for 2 months, 20% did partial breastfeeding, 20% did no breast feeding.
- MS treatments were in general restarted much earlier in non-breastfeeding group.
- Despite this there were less relapses in the exclusively breastfed group (38% vs 25%) in the first 6 months
- By the end of the year the relapse rates were similar again (as breast-feeding women stopped)
• Use of disease modifying treatment
o Formal recommendation is not to, however some agents are probably quite safe
o Use of IVIG as an interim measure was trialled (GAMPP study) with suggestion of a positive effect
IVF/Assisted reproductive therapy
• The use of GnRH agonists increased risk of relapse for 3 months following treatment
• GnRH agonists not frequently used in Australia
MS medications – evidence in pregnancy and breastfeeding
|
Drug and Pregnancy Category |
Evidence for pregnancy reccomendations |
Suggested Washout time |
Breast Feeding |
|
Interferons D (FDA-C) |
A large macromolecule with no significant
passage across the placenta Animal models show increased abortions but not
teratogenicity Avonex registry – 500 women
worldwide – No adverse effects Rebif registry – 425 women –
No adverse effects Systematic review (2012) – 761 pregnancies –
lower mean birth weight, shorter mean length and increased preterm birth. No association with low birth weight
(<2500g), congenital anomaly or spontaneous abortion. PI- If the patient becomes
pregnant or plans to become pregnant while taking interferon beta-1b, she
should be informed of the potential hazards and it should be recommended that
she discontinue therapy (Avonex adds: unless the
potential benefit justifies the potential risk to the foetus) |
1 month |
The levels of interferon beta-1a in breastmilk
are minuscule. In addition, because interferon is poorly absorbed orally, it
is not likely to reach the bloodstream of the infant. Six women on Avonex -
Milk samples from both breasts were collected after pumping with an electric
breast pump at 8 times after a dose at baseline and at 7 other times during
the first 72 hours after a dose. About half of the samples had undetectable
(<20 ng/L) amounts of drug. The highest concentrations were found at 1 or
4 hours after the dose in all women. The highest concentration found was 171
ng/L in one woman. Using this value, the authors estimated that the maximum
weight-adjusted dosage that an infant would receive is 0.006% of the maternal
dose. Likely
safe PI –
Because of the potential for serious adverse reactions in nursing infants, a
decision should be made whether to discontinue breastfeeding or Interferon
therapy TG-
Caution, insufficient data (Large molecular weight proteins/polypeptides are
unlikely to transfer into milk. In the absence of specific information,
adverse effects in the infant are unlikely) AMH - Should be safe
(interferons are not absorbed by the oral route). |
|
Copaxone B1 (FDA-B) |
A large macromolecule with no significant
passage across the placenta Animal studies – no ill effects Systematic review of 97 cases – no association
with obstetric complications or congenital abnormalities. Post marketing surveillance (Conference abstract
2003) 345 pregnancies 215 known outcomes 43 spontaneous abortions (20%) 9 elective abortions 1 ectopic pregnancy 155 live births 6 congenital anomalies (3.9% of live births) 90% had minimal/first trimester only exposure PI - Because animal reproduction studies are not
always predictive of human response, Copaxone should be used during pregnancy
only if clearly needed. |
1 month |
Undergoes rapid degradation to amino acids that
cannot be detected in the plasma, urine or faeces – unlikely to transfer
intact into breast milk (but has not been measured). Data on approximately 30 women breast feeding –
no adverse effects. Likely
safe PI -
caution should be exercised when Copaxone is administered to women who are
breastfeeding TG -
avoid, insufficient data AMH – No
human data |
|
Fingolimod D (FDA –C) |
Penetrates the CNS Animal models – increased malformations and
growth retardation. Exposure in clinical trials – 66 pregnancies –
5 congenital abnormalities (7.6%) – higher than would be expected. (219 exposed pregnancies, 5 malformations – CNS
drugs 2014 28:89) |
2 months |
No outcomes data at all. Excreted in the breast milk of rats Avoid PI –
Should not breastfeed. TG –
Avoid, insufficient data AMH - No human data;
avoid breastfeeding. |
|
Dimethyl Fumarate B1 (FDA-C) |
Animal data – at very high doses – reduced
foetal weight and delayed ossification.
Effects not evident at lower doses. Registry – 35 women exposed – no major adverse
events (however results not yet published) |
1 month |
No data on excretion into milk or outcomes
data. Avoid PI - A
risk to the newborn/ infant cannot be excluded. A decision must be made
whether to discontinue breastfeeding or to discontinue Tecfidera treatment.
The benefit of breastfeeding for the child and the benefit of treatment for
the woman should be taken into account. TG – No
entry AMH - No
data; avoid breastfeeding |
|
Teriflunomide X (FDA-X) |
Does not penetrate the CNS Animal data – high rate of congenital
abnormalities in rats and rabbits. Limited human data to date with leflunomide and
teriflunomide (7 pregnancies) has not detected any abnormalities. (59 exposed pregnancies – high elective
abortion rate, no major abnormalities - CNS drugs 2014 28:89) |
24 months (Consider washout) |
Passes into breast milk in animal studies (up
to 23% of the dose). No outcomes data for leflunomide or
teriflunomide. Avoid PI –
Avoid TG – No
entry AMH -
Avoid |
|
Natalizumab C FDA - C |
Probably crosses placenta Alpha-4 integrin receptors are expressed on
embryonic tissue Animal studies at high doses– decreased guinea
pig pup survival. Haematological
abnormalities in primates. Registry of 362 women exposed during pregnancy
– no adverse associations. Systemic review of 35 pregnancies – no adverse
associations. 9 women with severe disease treated throughout
pregnancy – reversible, mild-moderate haematological abnormalities in 8
newborns. |
1 month (3 had been previously recommended) |
Large protein molecule hence, the amount in
milk is likely to be very low and absorption is unlikely because it is
probably destroyed in the infant's gastrointestinal tract. No data on levels or outcomes. Use with
caution, especially in newborn/preterm. PI - the
potential for serious adverse reactions is unknown, a decision should be made whether to
discontinue breastfeeding or Tysabri therapy. TG -
Caution, insufficient data (Large molecular weight proteins/polypeptides are
unlikely to transfer into milk. In the absence of specific information,
adverse effects in the infant are unlikely) AMH - Detected in
breast milk; unlikely to be absorbed by child, however, manufacturer does not
recommend breastfeeding during treatment. |
|
Alemtuzumab |
139
pregnancies to date 2015 No
signal to increased abortion/malformation etc. |
|
Large protein molecule hence, the amount in
milk is likely to be very low and absorption is unlikely because it is
probably destroyed in the infant's gastrointestinal tract. No data on levels or outcomes. |
|
Daclizumab B3 FDA – C |
36 pregnancies to 2015 20 live
births – no abnormalities |
|
Large protein molecule hence, the amount in
milk is likely to be very low and absorption is unlikely because it is
probably destroyed in the infant's gastrointestinal tract. No data on levels or outcomes. |
|
Mitoxantrone D |
Adverse outcomes have been demonstrated in aminal studies and human cases. Avoid pregnancy for 6 months after treatment. |
6 months |
Avoid |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Steroids – Methylprednisolone and prednisolone. A FDA - No official category (Category C
suggested) |
Increased rate of cleft palate and lower birth
weight if used in the first trimester. Used in many women in second and third
trimester without any adverse effects. |
|
Low levels are excreted in breast milk. Advised to avoid breast feeding for 3-4hours
after a large intravenous dose to decrease exposure. No adverse effects have been reported. No adverse effects on ability to lactate have
been substantiated. TG -
caution with high pulse doses AMH – Nil
advice |
Effect of treatment on Relapse
Fragoso, Boggild et al. Effects of long-term exposure to DMD during pregnancy in MS. Clin Neurol and Neurosurg. 2013
• International database
• Compared women exposed (by definition to >8weeks, median 18weeks of treatment) to controls
• 37 GA
• 17 Interferon Beta
• IFN babies slightly smaller, otherwise no other significant differences (some of these women were probably included in previous meta-analysis).
• EDSS 45 months post pregnancy showed average increased EDSS in all groups
o Controls EDDS went from 1.39 to ~2.2.
• Probably a slightly lower post pregnancy EDDS in treated groups (however multiple confounding factors)
Hellwig et al. MS and pregnancy, experience from a nationwide database in Germany 2012.
• Treatment used in patient with worse disease (hence confounding results)
• However relapse rate post pregnancy was lower than pre-pregnancy in treated groups and higher post-pregnancy in non-treated groups.
• Defect rate:
o IFN 3/78 (3.8%)
o GA 2/41 (4.9%)
o No treatment 7/216 (3.2%)
•
Primary Progressive MS
Ocrelizumab
• ORATORIO trial (NEJM 376 Jan 2017)
• 732 patients, 488 active rx, 244 placebo
• 600mg infusion (300mg x2, 14 days apart), every 24 weeks for 120 weeks
• Primary end point – 12 weeks confirmed disability progression
o 32.9% vs 39.3% (Ocreliz vs placebo)
o HR 0.76 (CI 0.59-0.98)
o AbRR 6.4% NNT 15.6
• Less decline in 25 foot walk test on ocrelizumab
• No change in SF-36 physical component summary score
• The separation in the two groups appeared after first 12 weeks and then did not change.
Fingolimod
• INFORMS Trial
o Reduced lesion progression but not atrophy or function – negative trial
•
Secondary Progressive MS
Biotin (Vitamin B7/Vitamin H)
· ~150patients
· 12-15% of patients in treatment arm improved EDSS
· Mean overall EDSS improvement 0.1-0.2
· No side effects – except it interferes with thyroid assays
Natalizumab
· ASCEND trial – terminated due to lack of efficacy