Normal Pressure Hydrocephalus
Non-obstructive
enlargement of the ventricles in combination with one or more:
· Gait disturbance
· Urinary dysfunction
· Cognitive impairment
This
is referred to as Hakim’s triad (after Hakim and Adams who first described
condition in 1965)
Aetiology
• Idiopathic (iNPH)
• ‘Secondary’ NPH
o Trauma
o Meningitis
o SAH
N.B the identification of a secondary cause increases the likelihood
that shunting will be helpful
Clinical features
• Gait disturbance
o Slow short steps with reduced foot-floor clearance
o Outward angling of toes – gives shuffling appearance
o Difficulty turning – turn en bloc
o Decreased arm swing
o Patient may retain ability to carry out walking movements when lying down.
• Problems of control of urination – 50%
• Cognition
• Other symptoms sometimes seen:
o Upper limb tremor
Clinical rating scale – iNPH grading scale (developed by Japanese group)
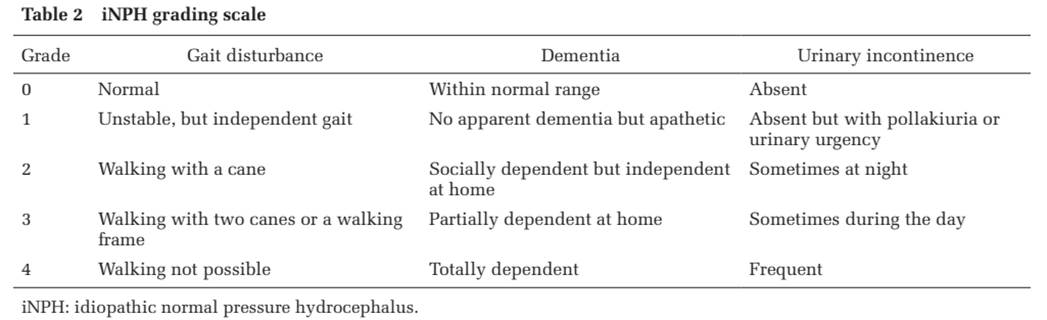
Diagnosis/Investigations
Imaging
NPH Radscale
score
Score >4 predicts higher chance of shunt responsive NPH
(From Kockum et al Plos One 2020)
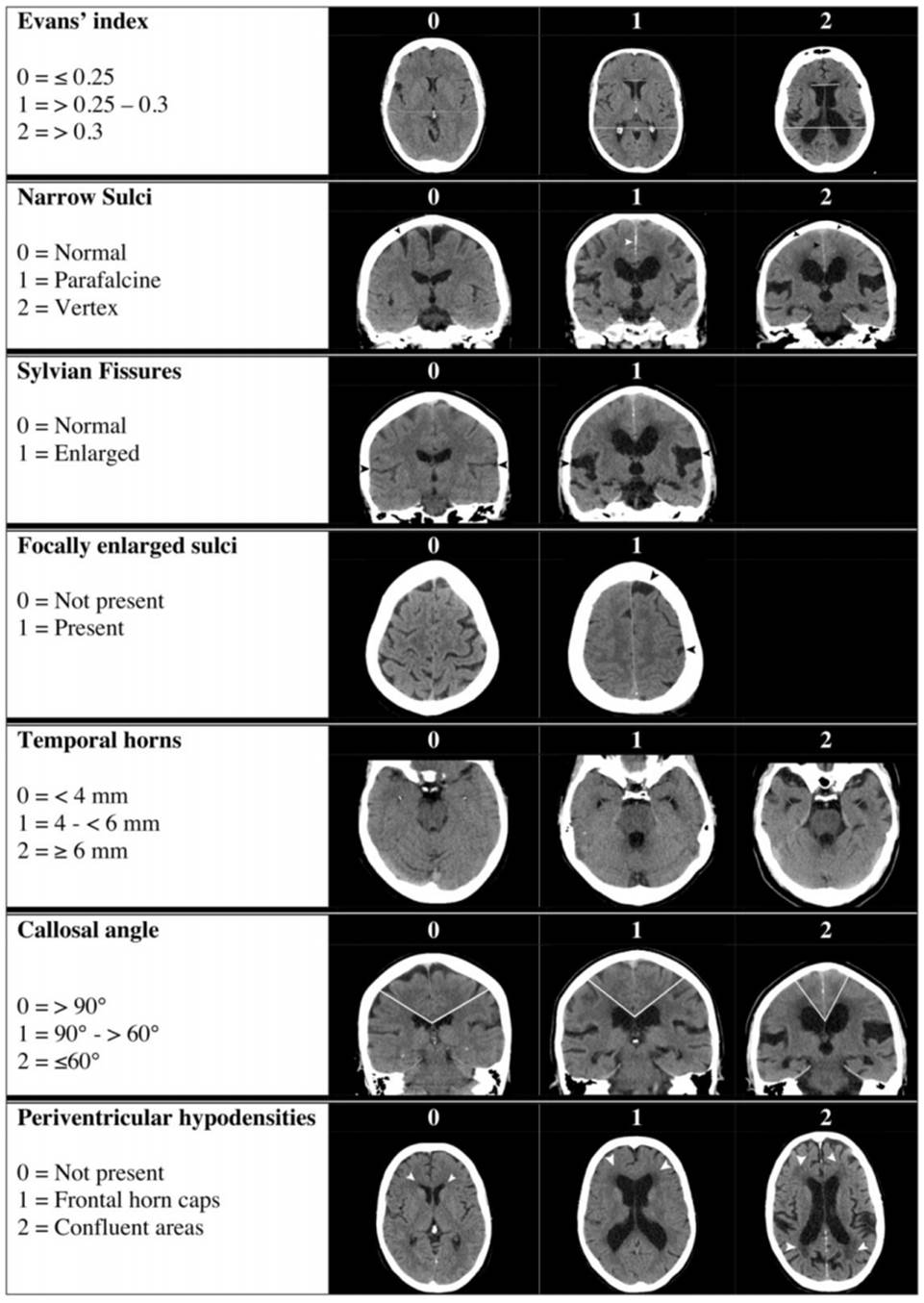
• Evan’s index
o Ratio of the widest width of the frontal ventricles to the widest width of the brain on an axial plane
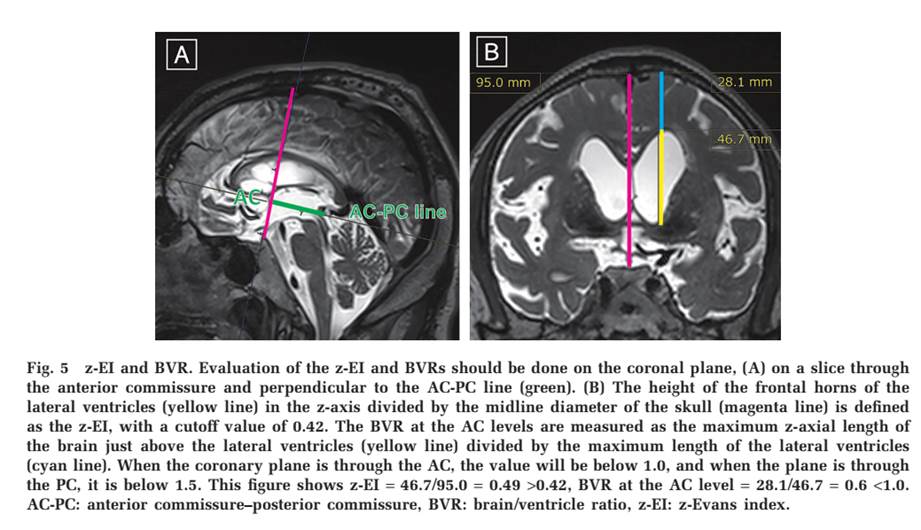
• Z-Axis Evan’s index and Brain-Ventricle ratio
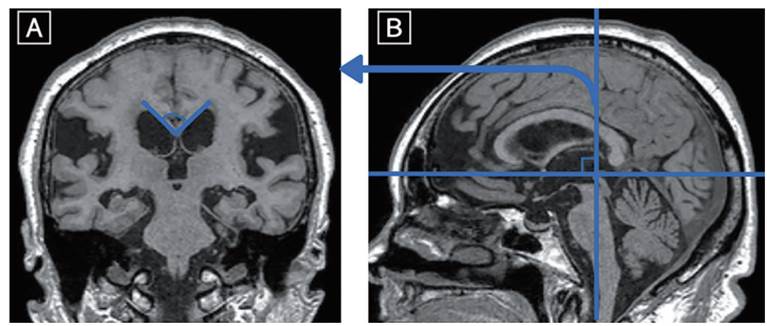
• Angle of corpus callosum on coronal imaging
• DESH – Dilated epidural spaces in hydrocephalus
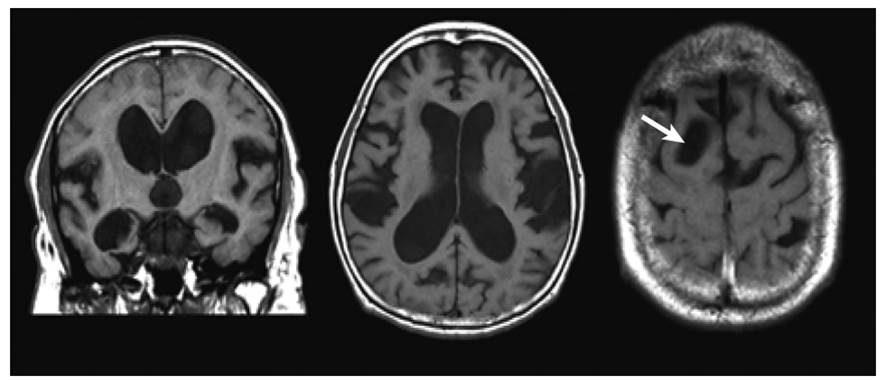
• Transependymal oedema
• Increased flow rate through aqueduct – phase contrast MRI measurement
o CSF flow velocity, pulsatile flow, stroke volume, and pressure gradient in the cerebral aqueduct significantly increase in iNPH.
o One study suggested very high accuracy, however not verified (Sensitivity 78–85%, Specificity 100%)
• Cingulate sulcus
o Measured in sagittal plane - In NPH the posterior part is narrower
Nuclear Medicine
• SPECT
o Convexity apparent hyperperfusion pattern (CAPPAH)
- Decreased blood flow in anterior cerebral hemisphere and around sylvia fissure, increased blood flow in high cortical areas
• FDG-PET
o Decreased glucose metabolism in basal ganglia suggested – but no consistent useful pattern?
Tap Test
• Measure CSF pressure (should be <20cm)
• CSF analysis - should be normal in NPH - abnormal composition may point to secondary cause (e.g. high protein)
• 30-50ml CSF drained
• Post testing at 2-4 hours (+/- 6, 8 and 24hours)
o Some suggest that improvements can occur over up to one week.
o UK centre use a single evaluation after 4 hours as most practical compromise.
o Gait tends to improve first. Cognition and urinary symptoms may also improve.
o
One study (Virhammar
et al. 2011) found that of patients that did respond 60% responded at 2 hours
with 96% having responded with in 8hours (100% responded by 24hours by
definition).
• Testing pre and post
o Gait testing
- 10m walk test – time or number of steps
• Positive test = 10% improvement on both or 20% improvement on one.
- Timed up and go (TUG)
- Video gait review (Gait style 1-8 (Normal through to wheelchair bound)
o iNPH rating scale (see above)
o Cognitive testing could be considered – MMSE (but unlikely to change acutely)
• Accuracy
o Sensitivity 58% (26-87%), Specificity 75% (33-100%)
o PPV estimated in one study at 72% for gait assessment alone and 91% when neuropsychological assessment added.
Continuous external lumbar drainage
• 24-72hours of lumbar drainage at 10ml/hr through temporary lumbar drain.
• Improved specificity diagnostic accuracy
• Risk of meningitis
Lumbar infusion study
• Fluid infused into CSF at one level and measured at another.
• Rate of CSF absorption is calculated
Biomarkers
• Still under investigation
• p-tau and t-tau – lower than in alzheimers disease
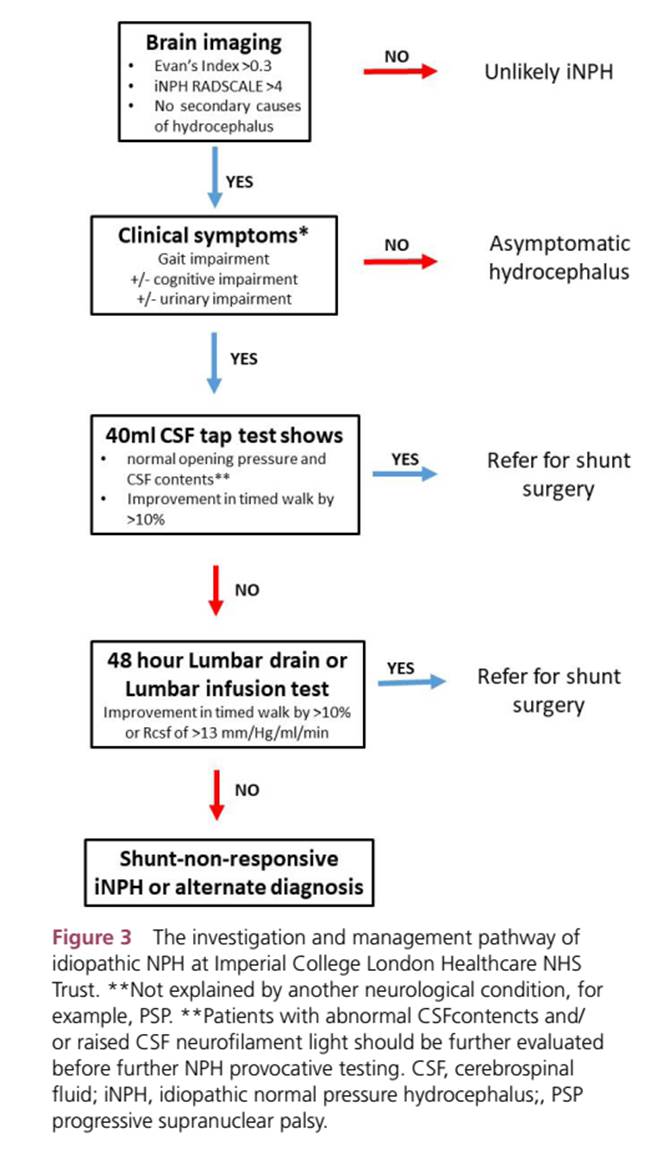
Diagnostic and treatment algorithm
UK group (Practical Neurology 2023)
Treatment/Prognosis
Suggested
that:
Improvement
in mRS
3-6
months – 39-81%
1
year 63-84%
Gait
improvement 60-77%
Cognitive
improvement 61-69%
Urinary
incontinence 52%
Co-morbidiites significantly affect prognosis
Keifer
index >4 predicts low chance of sustained improvement in function post shunt