Stroke Management Summary – Cairns Hospital (2020)
Acute blood pressure management

Bruce Campbell MJA 2019
(Acknowledgement to Dr Raka Datta for development of first
draft)
Acute Treatment
|
|||
|
|
Recommended
intervention |
Statistics |
Evidence/Papers/Guidelines |
Thrombolysis
|
Within 4.5hrs of symptom onset – consider IV thrombolysis (Alteplase) for patients with potentially disabling ischaemic
stroke (NIHSS >4) who meet eligibility criteria. |
Alteplase within 4.5hrs: Absolute increase disability-free survival - 10% if within 3hrs, 5% if within 3-4·5hrs Absolute increased risk
death 2’ ICH - 2% |
Meta-analysis: Effect of treatment delay, age, and stroke severity on the effects of
intravenous thrombolysis with alteplase for acute ischaemic stroke Emerson et
a (LANCET, 2014) |
|
|
Within 9hrs* of symptom onset –
Consider IV thrombolysis (Alteplase) for patients with: -
potentially
disabling ischaemic stroke (NIHSS 4-26) -
who meet
standard eligibility criteria AND -
salvageable
regions on CTP defined as: · vol. hypoperfusion/vol.
of ischemic core ratio >1.2 AND · absolute
difference > 10 ml AND · ischemic-core
< 70 ml. *
If wake-up stroke 9hrs from mid-point of sleep. |
Alteplase within 9 hrs vs. placebo: Adj RR 1.44, 95% CI 1.01-2.06, p value 0.04 |
EXTEND study (NEJM 2019) Primary outcome of mRS scale 0-1 at 90 days
assessed after receiving Alteplase between 4.5-9 hours post stroke onset on awakening
with stroke (if within 9 hours from the midpoint of sleep). Perfusion lesion–ischemic core mismatch was defined as: -
ratio > 1.2 between
the volume of hypoperfusion/volume of ischemic core AND -
absolute difference
> 10 ml AND -
ischemic-core < 70
ml. |
|
Alteplase for unknown
timeframe of stroke and selected MRI findings vs. placebo: Adj OR 1.61, 95%
CI 1.09-2.36, p value 0.02 |
WAKE-UP study (NEJM 2018) Primary outcome of mRS scale 0-1 at 90 days after
receiving Alteplase for unknown time of onset of stroke with MRI DWI evidence
of ischaemic stroke but no parenchymal hypointensity on FLAIR. (Large >1/3 MCA DWI excluded) |
||
Endovascular
clot retrieval
|
Within 6 hours of onset ECR should be considered for all patients with
ischaemic stroke who: -
Procedure
can commence within 6 hours of onset AND -
Have large
artery occlusion of anterior circulation (ICA/M1) ** This is not available in Cairns in this timeframe** |
ECR reduced mRS disability at 90 days. adj cOR
2·49, 95% CI 1·76–3·53,
p<0·0001. NNT 2·6 |
HERMES collaboration pooled date from 5 trials between 2010-2014
MRCLEAN, ESCAPE, REVASCAT, SWIFT PRIME, EXTEND IA. Trials assessed proximal
anterior circulation ischaemic strokes - ECR within 12hrs vs. control.
Primary outcome - mRS at 90 days. |
|
6-24 hours from onset ECR should be considered for all patients with
ischaemic stroke who: -
Procedure
can commence within 6-24 hours of onset AND -
Have large
artery occlusion of anterior circulation (ICA/M1) AND -
Have
salvageable tissue on perfusion imaging o Core <50ml o Penumbra >15ml o Mismatch ratio >1.8 Possible exclusion: Premorbid MRS >2 ASPECTS <6 or >1/3 MCA affected on CT*
(*see RESCUE-Japan) |
ECR 6-16hrs: Better mRS score, OR 2.77, p < 0.001 and functional independence 45%
compared to control 17%, p < 0.001 Trend to greater benefit with later, more severe
strokes. No difference based on age or
ASPECTS |
DIFFUSE 3 Study (NEJM 2017) ECR within 6-16hrs for occluded ICA (cervical or intracranial)
or proximal MCA with findings on CTP: -
Core
<70ml -
Ratio
penumbra/core > 1.8 -
Penumbra
>15ml NIHSS >/= 6 Premorbid MRS </= 2 Exclusion – ASPECTS <6 Primary outcome - mRS at 90 days |
|
|
ECR 6-24hrs: mRS in ECR group 5.5 vs. 3.4 in control. FI at 90 days 49%
ECR, 13% control No significant
difference in benefit b/n subgroups, age, NIHSS, time (<12 vs >12hrs) |
DAWN Study (NEJM 2018) ECR 6-24hrs for occluded intracranial
ICA/proximal MCA stroke + mismatch on CTP. -
Group A -
Age >80, NIHSS >10, Core <21ml -
Group B -
Age <80, NIHSS >10, Core <31ml -
Group C -
Age <80, NIHSS >20, Core 31-51ml Premorbid MRS 0 or 1 (i.e.<2) Exclusion – CT evidence of >1/3rd
MCA involved Primary outcome – utility weighted mRS +
functional independence (FI) at 90 days |
||
|
Primary outcome: ECR 31% vs Medical 12.7%. sICH: ECR 9% vs Medical 4.9% |
RESCUE-Japan LIMIT (NEJM 2022) ECR 6-12hours with large ischaemic area (ASPECT
3-5) Used unusual mixture of CT and MRI criteria Primary outcome: mRS 0-3 at 90 days |
||
ECR for Basilar
thrombosis
|
Consider for patients presenting up to 24 hours
with: -
PC-ASPECTS
score >6 -
NIHSS
>10 (may consider >6) -
Premorbid
mRS <3 |
Good functional outcome (mRS 0-3) at 90 days -
46% vs 23%. ARR 23%, NNT 4.3 |
ATTENTION trial (NEJM 2022) -
0-12 hours |
|
Good functional outcome (mRS 0-3) at 90 days -
46% vs 24%. ARR 22%, NNT 4.5 |
BAOCHE trial (NEJM 2022) -
60-24
hours |
||
|
|
|
|
|
|
Acute Treatment - Continued |
|||
|
|
Recommended
intervention |
Statistics |
Evidence/Papers/Guidelines |
Antiplatelet
|
Patients with acute ischaemic stroke should be
given Aspirin as soon as possible (ideally within 48hrs of onset). |
Fewer recurrent strokes in 14/7 (p < 0.001) In 14/7: 11 fewer deaths per 1000 treated In 6/12: 10 fewer deaths per 1000 treated Fewer recurrent strokes in 4/52 (p 0.01) In 4/52: 6.8 fewer deaths per 1000 treated On DC: 6.4 fewer deaths/dependency per 1000 treated In 3/52: 9 fewer cases of stroke or death in
hospital per 1000 treated |
IST study (LANCET 1997): Aspirin 300mg for 14 days vs. placebo. Primary
outcomes assessed at 14 days and 6 months CAST study (LANCET 2007): Chinese population only. Aspirin 160mg for 4
weeks vs. placebo. Primary outcome – death from any cause in 4 weeks, death
or disability on discharge IST+CAST pooled data |
Blood pressure
management
|
Patients for thrombolysis should have
BP reduced to <185/110mmHg before treatment and in first 24 hours
after treatment. Non-lysis patients with BP > 220/120 mmHg should have
BP cautiously reduced (e.g. by no more than 20%) over the first 24
hours. |
Mean SBP target in 3 separate groups did not
alter outcome for patients. 51%, 52%, 39% (p value 0.27). Odds of good
outcome greatest in group 2 (SBP 161-180mmHg) No difference in primary outcome in those given
GTN vs. placebo. Adj OR poor outcomes 1.25, 95% CI 0.97-1.60, p = 0.08 |
MAPAS study (NeuroCrit Care 2019) Patients divided into 3 groups for SBP management
in first 24hrs post ischaemic stroke. Group 1 140-160 mmHg, Group 2 161-180
mmHg, Group 3 181-200 mmHg RIGHT-2 study (STROKE 2019) Paramedic trial of stroke within 4hrs (using
FAST) + SBP >120mmHg receiving GTN vs. placebo. Primary outcomes – mRS 90
days. |
DVT prophylaxis
|
Chemical prophylaxis recommended -
Enoxaparin
is the preferred choice. |
Unfractionated heparin vs. enoxaparin: Enoxaparin reduced VTE by 43% compared to heparin
28%, RR 0.57, 95% CI 0.44-0.76, p = 0.0001 Risk of bleed similar in both groups |
PREVAIL Study (STROKE 2008) Unfractionated heparin vs. enoxaparin within
48hrs of ischaemic stroke. Primary outcomes – symptomatic/asymptomatic DVT,
symptomatic or fatal PE. |
|
Intermittent Pneumatic Compression – is also
effective |
Use of IPC: VTE occurred in 8.5% compared to
12.1% in control. ARR 3.6%, RRR 0.69. No significant difference in skin
breaks/falls. IPC patients had improved survival at 6 months |
CLOTS 3 Study (LANCET 2013) Intermittent pneumonic compression (IPC – similar
to SCUDS) applied to those with ischaemic stroke within 3 days. Primary
outcome – silent/symptomatic DVT |
|
|
NOT RECOMMENDED - TED/Compression stockings |
No significant improvement in DVT, increased risk
of skin complications |
CLOTS 1 Study (Lancet 2009) |
|
Investigations/ Interventions
|
|||
|
|
Recommended
investigation |
Statistics |
Evidence |
Imaging - Acute
|
CT Brain (non-contrast) For all patients suspected of acute stroke. |
Primarily to determine haemorrhagic cause or
established infarct. |
|
|
Acute CT Angiogram (arch – cerebral vertex) For all patients who are potential candidates for
ECR. MR Angiogram Consider if CI to CTA |
To assess intracranial large vessel occlusion and
state of proximal vessels for access. Can also be considered – however harder to do and
le |
|
|
|
CT Perfusion Brain Patients who are candidates for ECR or delayed
(>4.5hrs) IVTPA should have CTP to guide eligibility. |
|
|
|
|
MRI |
|
|
|
Imaging -
subacute
|
CTA/Carotid Doppler/MRA For patients with carotid territory symptoms who
are candidates for carotid revascularisation |
CTA/MRA allow imaging of rest of vascular tree to
assess for alternative aetiology Carotid Doppler may be more accurate for
quantification of significant stenosis MRA can be combined with Fat sat T1 imaging to
confirm arterial dissection |
|
Heart Rate
Monitoring
|
24 hours Telemetry/Holter Consider in all stroke patients |
|
Australian Stroke Guidelines 2017 |
|
Loop Recorder Consider in ESUS/Cryptogenic stroke |
Long-term monitoring: AF detected 8.9% vs. 1.4% control. HR 6.4, 95% CI
1.9-21.7, p < 0.001. Long-term monitoring: AF detected 16% vs. 3.2%
control. 95%
CI, 8.0-17.6, p<0.001. AF >2.5mins 9.9% vs 2.5% control |
CRYSTAL AF study (NEJM 2014) Long-term cardiac monitoring vs. conventional
measures in those with cryptogenic stroke. Primary outcome – time to first
detecting AF (>30sec) 6 months EMBRACE study (NEJM 2014) Long-term cardiac monitoring vs. control in those
with cyptogenic stroke/TIA in last 6 months. Primary outcome – time to first
detect AF (>30sec) in 90 days |
|
Echo-cardiography
|
TTE should be considered in cryptogenic strokes
and TIA as most cost effective option. TOE remains gold standard. |
Sensitivity to detect LA thrombus with TTE 0.79
and specificity 1 compared to TOE. |
Systemic Review – Routine echocardiography in the management of stroke and TIA. Economic analysis of both TTE + TOE for
stroke work up assessed. (Holmes et al, 2014). |
|
TTE with bubble study should be performed to
detect PFO in young patients (<60yrs) without alternative aetiology |
|
|
|
Bloods
|
Routine bloods: FBC, electrolytes, renal function, cholesterol and glucose levels.
Consider HbA1c if lacunar stroke/vascular risk factors/high blood sugar
levels “Young stroke bloods” – looking for
vaculitis/thrombotic causes should be considered in those < 50 years old
with minimal risk factors |
|
Australian Stroke Guidelines 2017 |
|
|
|
|
|
Secondary prevention
|
|||
|
|
Recommended
intervention |
Statistics
|
Evidence/Papers |
Antiplatelets
|
Acute
ischaemic strokes not thrombolysed should receive antiplatelet therapy in
first 24hrs – once haemorrhage excluded. Different antiplatelet
options/trials below. Australian
Stroke Guidelines 2017 |
||
|
Aspirin
alone |
Aspirin
lifelong after ischaemic stroke/TIA |
Reduced recurrent stroke 60%, HR
0·42, 95% CI 0·32–0·55, p<0·0001 and disabling/fatal stroke 70% HR 0·29, 95% CI 0·20–0·42, p<0·0001.
Greatest benefit in TIA/minor stroke patients. |
Meta-analysis: Effect of aspirin on risk and severity of early
recurrent stroke after TIA and ischaemic stroke: time course analysis of
randomised trials - 12
trials of aspirin vs control data pooled - Outcomes regardless of dose, aetiology of stroke - Rothwell
et al (LANCET 2016) |
Clopidogrel
vs. Aspirin
|
Clopidogrel
slightly better than aspirin in long term secondary prevention (more evidence
to use DAPT in first 3/52 – see below trials) |
Clopidogrel
vs. Aspirin Relative
RR 7% with clopidogrel (p 0.043). No major differences in safety. |
CAPRIE
study (LANCET 1996) Clopidogrel
vs. aspirin to reduce risk of clinical thrombotic events (patients
followed for 3yrs). Primary outcome – Ischaemic stroke, MI and vascular
death. |
|
Aspirin +
Dipyrimadole (Asasantin) |
Asasantin
may be alternate to Aspirin. Risk of
headache with this combination. Requires slow up-titration. ** N.B.
Asasantin no longer available in Australia** |
Risk stroke or death
reduced: 13% aspirin (p =
0.016), 15% dipyridamole (p = 0.015), 24% combination therapy (p < 0.001). |
ESPS-2 (J
Neurol Sci 1998) Patients with prior stroke/TIA
randomized to aspirin alone (50 mg daily), modified-release dipyridamole
alone (400 mg daily), the two agents in combination, or placebo. Primary
outcomes – stroke or death. |
|
Clopidogrel
vs. Asasantin |
Clopidogrel
is similar to but not better than Asasantin in preventing recurrent strokes. ** N.B.
Asasantin no longer available in Australia** |
Clopidogrel
vs. Asasantin Recurrent
strokes 9% Asasantin, 8.8% - Clopidogrel. Secondary outcome 13% each group. |
PRoFESS
study (NEJM 2008) Clopidogrel
vs. Asasantin in those with recent ischaemic stroke. Primary outcome – first
recurrent stroke. Secondary outcome – stroke/MI/death from vascular causes.
Patients followed for mean 2.5yrs |
|
Clopidogrel
+ Aspirin |
Give aspirin plus clopidogrel
within 24hrs of ischaemic stroke and use: -
short term (3/52) -
in minor ischaemic stroke
(NIHSS</=3) OR -
high-risk TIA (ABCD >/=4) Long term use of combination should NOT be
routine in stroke secondary prevention (may be used in selected cases or if
co-morbid IHD/stents) Australian
Stroke Guidelines 2017 |
Clopidogrel
+ aspirin: Major
ischaemic events 5% vs. aspirin alone 6.5% HR 0.75, 95% CI 0.59-0.95, p =
0.02 Clopidogrel
+ aspirin: Major
bleed 0.9% vs aspirin 0.4% HR 2.32, CI 1.10-4.87, p = 0.02 Risk of
haemorrhage increased after 30 days with minimal further benefit. |
POINT
study (NEJM 2018) Clopidogrel
and Aspirin given for for minor acute ischaemic stroke (NIHSS </=3) or
high risk TIA (ABCD2 >/= 4). Primary outcome – risk of major recurrent
stroke, MI, death from vascular event at 90 days. |
|
Clopidogrel
+ aspirin: Stroke
8.2% vs aspirin alone 11.7% HR 0.68,
95%CI 0.57-0.81, p < 0.001 Mod-severe
haemorrhage 0.3% both groups |
CHANCE
study (NEJM 2013) Chinese
population only. Clopidogrel and Aspirin given for minor acute ischaemic
stroke (NIHSS </=3) or high risk TIA (ABCD2 >/= 4). Primary outcome –
stroke (ischaemic or haemorrhagic) during 90 days |
||
|
Clopidogrel
+ aspirin: Stroke
15.7% vs. clopidogrel alone 16.7%. RRR 6.4% (95% CI -4·6- 16·3), ARR 1% (95%
CI −0·6-2.7) Non-significant
difference. Clopidogrel
+ aspirin: Increased risk of major bleeds, no difference in mortality |
MATCH
study (LANCET 2004) Clopidogrel
and Aspirin for up to 18 months in those with recent ischaemic stroke vs.
Clopidogrel only. Primary outcome – recurrent stroke, MI, vascular death,
rehospitalisation for ischaemia. |
||
|
Clopidogrel + aspirin: Reduced
recurrent stroke by 20 in 1000. Increased mod-severe bleeding by 2 in 1000. |
Meta-analysis: pooled data from all three trials – Clopidogrel
+ aspirin for minor stroke and high risk TIA most beneficial with minimal
harm in first 21days |
||
Blood
pressure management
|
Patients
with recent stroke or TIA and ongoing BP of > 140/90mmHg should have long
term BP lowering therapy initiated. Ideal
long-term BP aim not well established. Target SBP
< 130mmHg may achieve greater benefit especially in strokes due to small
vessel disease. |
Higher BP
target vs. lower target: No
significant reduction in all strokes HR 0.81, 95% CI 0.64-1.03, p = 0.08.
Rate of ICH reduced in lower target group p = 0.03 Intense BP lowering significantly reduced risk of stroke [RR 0.71
(0.60-0.84)], major cardiovascular events [0.75 (0.68-0.85)] |
Australian
Stroke Guidelines SPS 3
study (LANCET 2013) Patients
with recent lacunar strokes assigned to SBP targets of 130-149mmHg or less
than 130mmHg. Primary outcome – reduction in all strokes (ischaemic and
haemorrhagic). Assessed at 1 year. Meta
Analysis: Effect of
BP lowering on outcome incidence in hypertension: effects of more vs. less
intensive BP lowering and different achieved BP levels (Thomopoulos et al,
2016) – multiple RCTs assessed |
Lipid
management
|
Patients
with ischaemic stroke and possible atherosclerotic contribution should have
high dose statin if there is reasonable life expectancy. New
evidence to aim LDL < 1.8. Fibrates
are not routinely recommended for stroke prevention Statins are
not routinely recommended for haemorrhagic strokes |
Atorvastatin
vs placebo: 11% on
atorvastatin vs. 13.1% on placebo had fatal/non-fatal stroke. ARR 2.2%, adj
HR 0.84, 95% CI 0.71-0.99, p = 0.03. LDL target
of 1.8mmol/L vs. 2.3-2.8mmol/L vascular events 8.5% in lower target and 10.9%
in higher target. Adj HR 0.78, 95% CI 0.61-0.98, p = 0.04 |
Australian
Stroke Guidelines SPARCL
study (NEJM 2006) Patients
with stroke/TIA in last 6/12 and LDL 2.6-4.1mmol/L assigned to atorvastatin
vs. placebo. Primary outcome - first non-fatal/fatal stroke. Median follow up
4.9 years. Comparison
of two LDL Cholesterol targets after ischaemic stroke (NEJM 2020) France +
South Korea population. Patients with ischaemic stroke/TIA in last 3/12 had
LDL targets of 1.8mmol/L vs. 2.3-2.8mmol/L. Primary outcome – major vascular
event (stroke, MI, CVS death) |
Carotid
surgery
|
Carotid
endarterectomy recommended for recent (<3 months) non-disabling carotid
artery territory ischaemic stroke/TIA if ipsilateral carotid stenosis
measures 70-99% Carotid
endarterectomy should be preformed as soon as possible (ideally within 2/52)
after ischaemic stroke/TIA - Based on
subgroup analysis |
Carotid
surgery vs. control: Stroke/death
37% surgery vs. 36.5% control. Stenosis >80%, stroke/death at 3yrs 14.9%
surgery vs. 26.5% in control. CEA vs. control: reduced 5-year risk of death or
stroke by 29% for symptomatic high-mod (50-69%) carotid stenosis |
ECST study
(LANCET 1998) Patients
with some degree of carotid stenosis and transient of minor strokes in
distribution of carotid arteries in the last 6/12, had surgery vs. control.
Primary outcome – major stroke or death. NASCET
study (STROKE 1999) Patients
with symptomatic carotid stenosis: low-moderate (<50%), high-moderate
(50-69%) and severe (>70%) given CEA vs. control. |
|
CEA can be
considered in selected patients with recent (<3 months) non-disabling ischaemic
stroke or TIA patients with symptomatic carotid stenosis of 50–69% |
|
|
|
|
Carotid
Endarterectomy preferred over Carotid Stenting in general |
Stenting
vs. CEA: increased peri-procedural outcomes (MI, stroke, death) with
stenting, OR 1.31, 95% Ci 1.08-1.59 |
Meta-analysis - Carotid Artery Stenting vs. Carotid
Endarterectomy, 13 RCTs (2011). Peri-procedural outcomes, intermediate and
long term outcomes assessed. |
|
|
|
|
|
|
Anticoagulation
for AF
|
Anticoagulation
recommended for patients with ischaemic stroke/TIA with AF (paroxysmal or
permanent) - DOAC
over warfarin in non-valvular AF - No
preferences between DOACs |
Indirect comparison
Apixaban, Dabigatran, Rivaroxaban: similar efficacy with all three in stroke
prevention. Reduced haemorrhagic stroke dabigatran vs. rivaroxaban HR 0.15, 95% CI 0.03-0.66 |
Primary
and secondary prevention with new oral anticoagulant drugs for stroke
prevention in AF: indirect comparison analysis. Primary outcome – secondary prevention of
stroke. -
Rasmussen et al (BMJ 2012) (Trial of
each DOAC vs. warfarin for stroke prevention: RELY, ARISTOTLE, ROCKET-AF) |
|
Restarting after ICH |
See ICH section
below |
|
|
PFO
closure
|
Recommended
in patients -
aged <
60 -
non-lacunar
stroke -
no other
aetiology for stroke found. AF risk
slightly increased with PFO closure |
Summary: Overall
benefit of closure with long term follow-up.
All trials demonstrated low risk of recurrence in young patients with
cryptogenic stroke. Risk of recurrence is late (c.f. carotid disease). All except DEFENCE-PFO use age limit for
60yrs. |
Summary
major trials: Patent
Foramen Ovale - story closed (Kohrmann
et al, 2019) (GORE-REDUCE,
CLOSE, DEFENSE-PFO, RESPECT) |
ICH
|
|||
Acute
blood pressure management
|
Acute reduction
of BP to around 140 (but not significantly below): -
is safe -
reduces
haematoma expansion -
has no
effect on mortality -
trend to
reduced disability |
No
benefit. Death or
disability 38.7% vs 37.7% (RR 1.04, CI 0.85-1.27) |
ATACH-2
Trial (NEJM 2016) ICH
(<60mm) and GCS >5 randomised to BP 110-139 vs BP 140-179. Within 4.5 hours of onset. Achieved mean BP
was 129 vs 141. |
|
Trend to
benefit. Death or
disability 52% vs 55.6% (HR 0.87 CI 0.75-1.01). Analysis
of mRS outcomes showed slight shift to improved outcomes. |
INTERACT2
NEJM 2013 ICH randomised to BP <140 within 1 hour vs
std care with targe <180. Within
4.5 hours of onset. Achieved mean BP was ~140 vs 150. |
||
|
3 month
mortality OR 0.99 (CI: 0.82-1.2) 3 month
death or dependency OR 0.91 (CI: 0.8-1.02) ICH
expansion OR0.82 (CI:0.68-1.00) |
Meta-analysis (Boulouis JNNP 2017) |
||
|
|
Caution if
initial BP >220mmHg, consider less aggressive target. |
Patients
with initial BP >220mmHg treated with intensive BP management (vs standard
BP control) had higher rate of neurological deterioration (15.5 vs6.8%) and
renal AE 13.6% vs 4.2%) with no difference in disability or death. |
ATACH-2
subgroup (JAMA Neurol 2020) |
|
Restarting
antiplatelets after ICH |
|
Recurrent
sICH -
4% (antiplatelet)
vs 9% (avoid) – after 2 years -
8.2% vs 9.3% - after 3 years Ischaemic
stroke 7% vs 10% - after 2 years Major
vascular event – 26.8% vs 32.5% Overall no
significant differences – trends to improved outcomes with restarting. |
RESTART
trial Lancet 2019 Patients
taking antiplatelet or anticoagulant who had ICH Restart
antiplatelet vs avoid 268pts
each group. Started at median ~70-80
days post event. Median F/U
2 years RESTART
trial 3yr F/U JAMA Neurol 2021 |
|
Restarting Anticoagulation after ICH |
No clear
recommendation |
Low rate
of recurrent ICH 8% (AC) vs 4% (no-AC) – NS Any
recurrent stroke (ICH or ischaemic) 11% vs 22% |
SoSTART
trial (Lancet Neurology 2021) ICH,
history of AF, CA2DS2-VASc at least 2 DOAC/Warfain
vs Avoid anticoagulation ~100
patients in each group Median
retart time 115 days post ICH |
|
Rapid Assessment |
|||
|
|
Recommended intervention |
Statistics |
Evidence/Papers/Guidelines |
|
History |
ROSIER Scale (score from -2 to 5) Scale contains pertinent history and examination
findings with negative/positive scores. Useful scale to suspect stroke/TIA Consider Stroke if score ≥ 1 |
Sensitivity 93% Specificity 83% PPV 90% |
NHMRC guidelines *APPENDIX 1 |
|
Clinical Assessment |
ACT-FAST Scale Scale contains pertinent examination findings to
prompt suspicion of large vessel occlusion Designed for pre-hospital/paramedic assessment however
useful to triage patients needing urgent CTA/CTP in ED |
Sensitivity 85% Specificity 88% PPV 96% |
(ACT-FAST)
algorithmic pre-hospital triage tool for endovascular thrombectomy: ongoing
paramedic validation – Zhao et al, BMJ 2018 *APPENDIX 2 |
|
|
NIHSS Score Rapid assessment to identify deficits due to
stroke. - Small stroke (NIHSS < 4) - Moderate stroke (NIHSS 5-15) - Moderate-Severe stroke (NIHSS 16-20) |
|
Australian Stroke Guidelines 2017 Strengths: Reliable tool to rapidly assess stroke deficits Limitations: Heavily weighted towards Left Stroke - 5 points for language Less weight on Posterior Circulation Strokes - Diplopia, vertigo, unsteady gait not assessed |
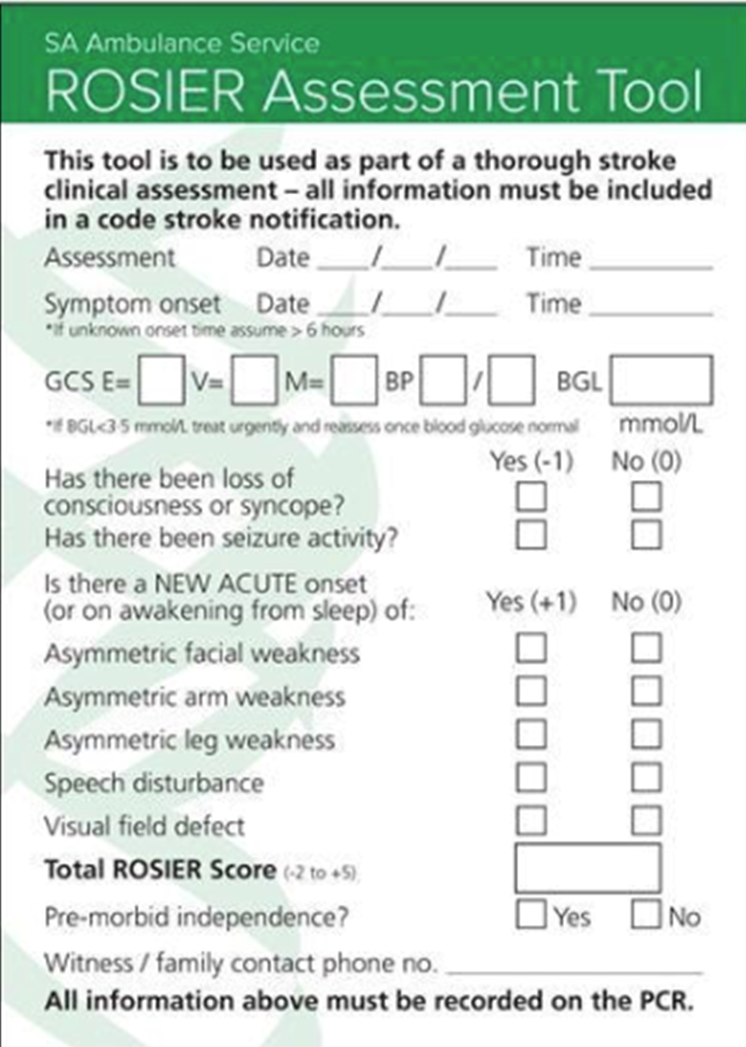 APPENDIX 1: ROSIER scale
APPENDIX 1: ROSIER scale
 APPENDIX 2: ACT-FAST scale
APPENDIX 2: ACT-FAST scale