Stroke Syndromes
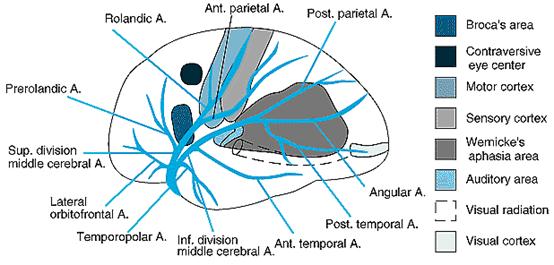
MCA stroke
Syndromes
- Complete
occlusion of MCA
- Contralateral
hemiplegia, hemianaesthesia, homonymous
hemianopia and gaze to the ipsilateral side
- Global aphasia
if dominant side
- Apraxia,
neglect, anosognosia if non-dominant
- Superior
division of MCA occlusion
- A combination
of sensory, motor and fluent (expressive, Brocca’s)
aphasia
- Inferior
division of MCA occlusion
- Wernike’s (fluent)
aphasia with superior quadrantanopia
- Lenticulostriate
- Pure motor or
motor-sensory stroke
- Genu – facial
weakness
- Arm then leg
are affected as ischaemia moves posteriorly

Anterior Cerebral
Artery
- Precommunal (A1) – joins
Carotid to anterior communicating
- Supplies
anterior portion of internal capsule, amygdala, anterior hypothalamus and
part of caudate nucleus
- Occlusion of A1
generally well tolerated to flow via communicating artery
- Unilateral
congenital atresia of A1 can occur so that occlusion of the contralateral
A1 results in bilateral ACA infarction
- Postcommunal (A2) – the ACA
after the communicating junction
- Occlusion can
result in :
- Foot and leg
paralysis or sensory loss
- Urinary
incontinence
- Abulia
- Gait apraxia
- Dyspraxia of
left limbs (corpus callosum)
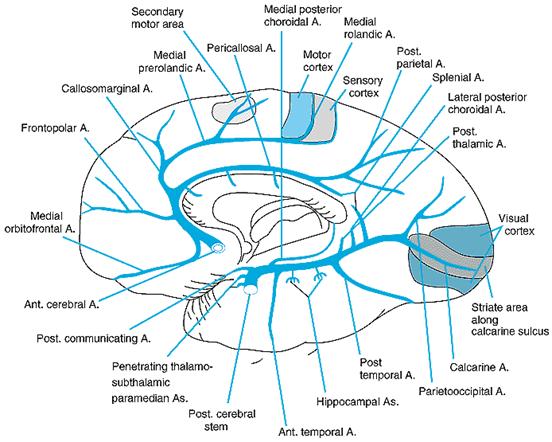
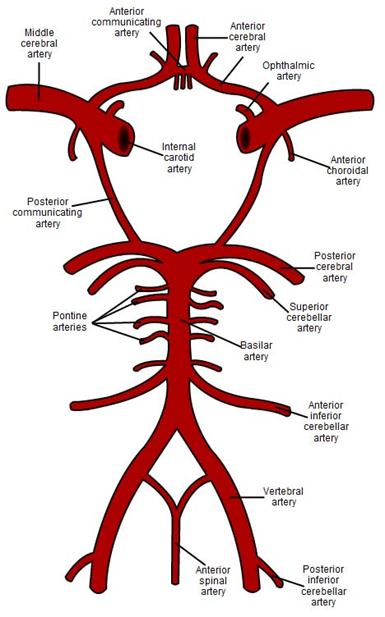
Posterior Cerebral
Artery
- 75% have
“normal” anatomy with PCA’s deriving from basilar
- 20% have one PCA
deriving from the internal carotid with atria of P1 (the segment between
basilar and junction with communicating)
- P1 syndromes
- Subthalamus,
thalamus
- Cerebral
peduncle and midbrain
- Third nerve
palsy plus contralateral ataxia (red nucleus) - (Claude’s syndrome)
- Third nerve
palsy plus contralateral hemiplegia (cerebral peduncle) (Weber’s syndrome)
- P2 syndromes
- Medial temporal
and occipital lobes
- Transient
memory problems can occur
- Visual defects
Thalamus
- Can be affected
by PCA infarct, hypertensive haemorrhage or venous infarction
- Sensory deficit
(all modalities) – contralateral
- Dominant
- Apahsia (with
preserved verbal repetition)
- Non-dominant
- Constructional
apraxia or mutism
Medullary Syndromes
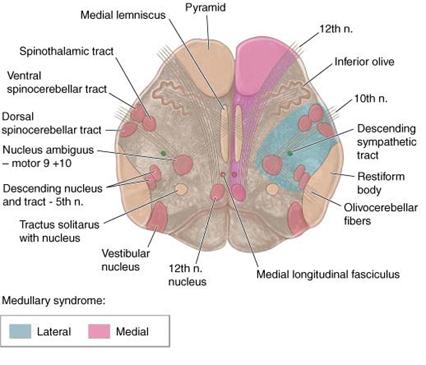
- Medial
- Ipsilateral
- Tongue
paralysis (12th nerve nucleus)
- Contralateral
- Paralysis of
arms and legs (sparing face) – pyramidal tracts, prior to decussation
- Loss of light
touch and proprioception – medial lemniscus
- Lateral
- Usually PICA
occlusion
- Ipsilateral
- Pain, numbness
and impaired sensation over half the face – 5th nerve
- Ataxia,
falling to side of lesion – probably spinocerebellar tract and part or
cerebellum
- Nystagmus,
diplopia, vertigo – vestibular nucleus
- Horner’s
syndrome – descending sympathetic tracts
- Dysphagia, hoarsness – 9th and 10th nerve
fibres
- Loss of taste
– nucleus and tractus solitarius
- Numbness of
ipsilateral arm, trunk or leg – gracile or cuneate nuclei
- Weakness of
face
- Contralateral
- Impaired pain
and temperature sensation – spinothalamic tract