Trigeminal
Autonomic Cephalgias
Trigeminal Autonomic Cephalgias
Definitions
- Primary
headache disorders characterised by short lasting headaches associated
with cranial autonomic symptoms
- Includes
- Cluster
headache
- SUNCT/SUNA
- Paroxysmal
hemicrania
- Common features
- Trigeminal
distribution of pain
- Ipsilateral
cranial autonomic features
Pathogenesis
- Pain
- Likely
results from activation of V1 division of trigeminal nerve
- Autonomic
effects
- Activation
of parasympathetic outflow (via facial nerve)
- Injury to
sympathetic outflow fibres
- Various
theories
- Vascular
activation
- Trigeminal
autonomic reflex
- Hypothalamic
activation – thought to be primary cause
- Secondary
causes
- A small but
definite proportion of patients have had structural brain lesions
identified as a cause (hence neuroimaging is recommended for all)
|
|
Cluster |
Paroxysmal hemicrania |
SUNCT/SUNA |
Migraine |
Trigeminal neuralgia |
|
Sex |
3M: 1F |
M=F |
1.5M :1F |
|
|
|
Pain |
|
|
|
|
|
|
Quality |
Sharp/stab/throb |
Sharp/stab/throb |
Sharp/stab/throb |
|
|
|
Severity |
Very severe |
Very severe |
Severe |
|
|
|
Distribution |
V1>C2>V2>V3 |
V1>C2>V2>V3 |
V1>C2>V2>V3 |
|
V1(10%) V2(35%) V3(30%) |
|
Attacks |
|
|
|
|
|
|
Freq (/day) |
1-8 |
20 |
100 |
<1 |
|
|
Length |
30-180 |
2-30 |
1-5 |
Hours |
|
|
Triggers |
|
|
|
|
|
|
Alcohol |
+++ |
+ |
- |
|
|
|
Cutaneous |
- |
- |
+++ |
|
|
|
Agitation /restlessness |
90% |
80% |
65% |
|
|
|
Episodic vs chronic |
90:10 |
35:65 |
10:90 |
|
|
|
Circadian periodicity |
Present |
Absent |
Absent |
|
|
|
Treatment effects |
|
|
|
|
|
|
Oxygen |
70% |
No effect |
No effect |
|
|
|
Sumatriptan |
90% |
20% |
<10% |
|
|
|
Indomethacin |
No effect |
100% |
No effect |
|
|
|
Migraine features with attacks |
|
|
|
|
|
|
Nausea |
50% |
40% |
25% |
|
|
|
Photophonia/ phonophobia |
65% |
65% |
25% |
|
|
|
|
|
|
|
|
|
Cluster Headache
Epidemiology
- ~0.1%
- M:F ~5:1 (85%
male)
- Onset in
teens – 20’s
- RF
- Family
history confers significant risk
Clinical manifestations
- Up to 8
attacks/day
- Strictly
unilateral during an attack
- Last 15min to
3hours
- Occur daily
for up to several weeks
- Rarely
chronic – over a year without remission
- Can shift
sides between different attacks in 15%
- Attacks often
nocturnal
- Alcohol can
be a trigger during a bout
- Patients
often restless, move about (c.f. migraine)
- Pain
- Severe
- Orbital,
supraorbital or temporal
- Autonomic
- Ptosis
- Miosis
- Lacrimation
- Conjunctival
injection
- Rhinorrhoea
- Nasal
congestion
- 3% of
patients lack autonomic symptoms
- Chronic
course in 10%
Diagnosis
• Clinical
• Imaging
• Should be done for
all new patients given the risk of secondary (i.e. structural) causes
Criteria ICHD-3
• Severe or very severe unilateral orbital, supraorbital and/or temporal pain lasting 15-180 min (when untreated)1
• Either or both of the following:
o At least one of the following symptoms or signs, ipsilateral to the headache:
- a) conjunctival injection and/or lacrimation
- b) nasal congestion and/or rhinorrhoea
- c) eyelid oedema
- d) forehead and facial sweating
- e) forehead and facial flushing
- f) sensation of fullness in the ear
- g) miosis and/or ptosis
o A sense of restlessness or agitation
• Attacks have a frequency between one every other day and 8 per day for more than half of the time when the disorder is active
Treatment
Avoid precipitants
• Alcohol
• Vasodilating drugs
• High altitude
Acute
• Oxygen
o High flow oxygen for at least 15min – proven effective – relieves 60-80%
o 7-12L/min – stop if no response in 15-20min, use for ~30min if response obtained.
o Continued use for ongoing attacks within a short period of time may be couter-productive
• Triptans
o Sumatriptan
- >75% response rate to 6mg s/c sumatriptan
- Can give up to two injections/day
- Some patients may respond to a smaller 3mg dose
- Intranasal (20mg) may have some benefit but much less effective than SC
o Zolmitriptan
- Intranasal 5-10mg – only 28% response rate
- Oral 5-10mg also a low response rate
o Other triptans – no evidence
• Lignocaine
o 1ml of 4-10% solution – dripped or sprayed into the nostril ~ 30% response rate
o Often not effective on its own, can be added as adjunct to other agents
o Applied with patient lying down, head back and rotated to affected side, remain there for 5min
• Ergots
o Intranasal not effective
o Oral may be of some benefit - 1-2mg
o IV DHE may be helpful in severe cases
• Octreotide
o Probably not effecitve
o Single dose of 100mcg s/c was effective in one trial (less than above Rx)
Short term prophylaxis
• Prednisolone
o PredCH Trial protocol – 100mg for 5 days, tapered by 20mg every 3 days (total 17 days)
• Greater occipital nerve block
o Depromedrol 40mg + 1-2ml of 2% lignocaine
o Trial evidence for betamethasone and triamcinolone (10mg)
Long term prophylaxis
• Verapamil
o Is the agent of choice
o 240-480mg/day, short acting preparation preferred (Max 960mg/day)
o 80mg tds increasing by 80mg every 2 weeks with ECG monitoring at each step.
• Lithium
o 600-1600mg/day
o Monitor blood levels, keep b/n 0.4-0.8nmol/L (lower than used for bipolar)
• Topiramate
o Some limited evidence
o Dose up to 100-200mg/day
• Galcanezumab
o Clinically small (but statistically significant effect).
• Valproate and Gabapentin
o Some anecdotal effectiveness however trials generally negative
• Melatonin
o 10mg/day (immediate release)
o Small trials with some positive effect
• Methylsergide – (Not available in Aust.)
o 1mg/day, increased to 12mg/day as tolerated
o Only to be used for max 3-4 months given potential for systemic fibrosis
o Methylergonovine is alternative
• Other agents that have been used and are probably not effective:
o Pizotifen, baclofen, clonidine, botox
Nerve Stimulation
·
Invasive and non-invasive VNS have been used with
some effect
·
DBS used in some cases
·
Occipital nerve stimulator effective in some case
reports/small series
Prognosis
- 80% of
patients continue to have attacks after 15years
References
Wei DY, Goadsby PJ. Cluster
headache pathophysiology - insights from current and emerging treatments. Nat
Rev Neurol. 2021 May;17(5):308-324. doi:
10.1038/s41582-021-00477-w. Epub 2021 Mar 29.
Paroxysmal
hemicrania
- Rare (3-6% of
trigeminal autonomic cephalgias)
- Female>male
- Onset 20-40
- Similar to
cluster but shorter attacks (2-30min)
- More frequent
attacks
- Less severe
autonomic features
- More often
chronic with out periods of significant
remission
- Complete
response to indomethacin within one week
SUNCT/SUNA
- Short-lasting
Unilateral Neuralgiform headache with Conjunctival injection and Tearing)
(SUNCT)
- Short-lasting
Unilateral Neuralgiform headache with Autonomic symptoms (SUNA)
- Rare
- Short
lasting, but frequent, severe, unilateral attacks associated with
autonomic features and which are often triggered.
- Similar to Trigeminal neuralgia in many ways
- Most data
from:
- Lambru G, Stubberud A, Rantell K, et al. J Neurol Neurosurg
Psychiatry 2021;92:233–241.
|
|
|
|
Onset age (mean) 43 |
|
|
Female 63% |
|
|
Onset age (range) 13-76yrs |
|
|
Site of pain (dec frequency) |
Periorbital Cheek Temporal Retroorbital Forehead Occiput Jaw |
|
Laterality |
Right ~50% Left ~40% Side variable (10% |
|
Mean daily frequency (range) |
44 (1-250) |
|
Mean attack severity (out of 10) |
9 |
|
Autonomic features: |
Conjunctival injection and lacrimation (distinguish SUNCT from SUNA) Rhinorrhoea (30-50%) Ptosis (23-50%) Facial flushing (~40%) Aural fullness (20%) |
|
Mean attack duration (sec) |
170 (range: 1-1200) |
|
Course |
Episodic 10% Chronic 90% |
|
Triggerability |
Triggered 5% Spontaneous 36% Both 57% |
|
Trigger factors: |
Chewing/eating Cold wind Light touch Brushing teeth |
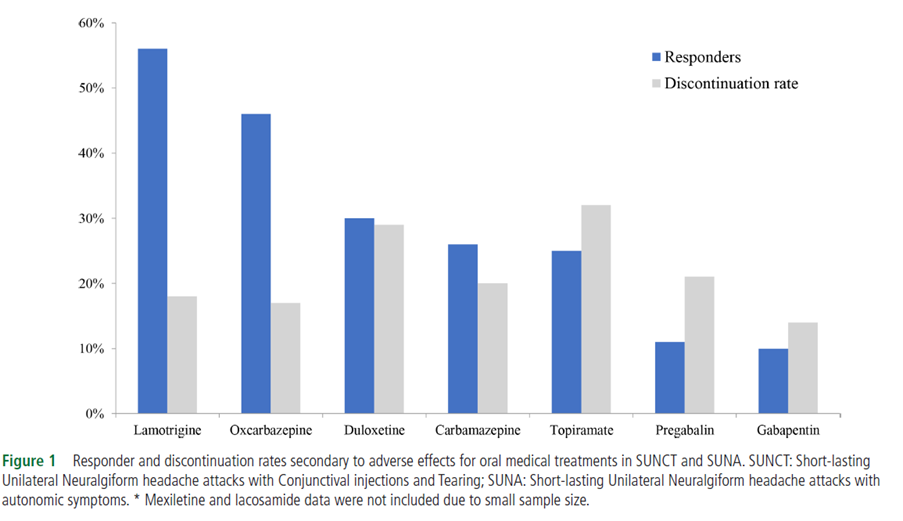
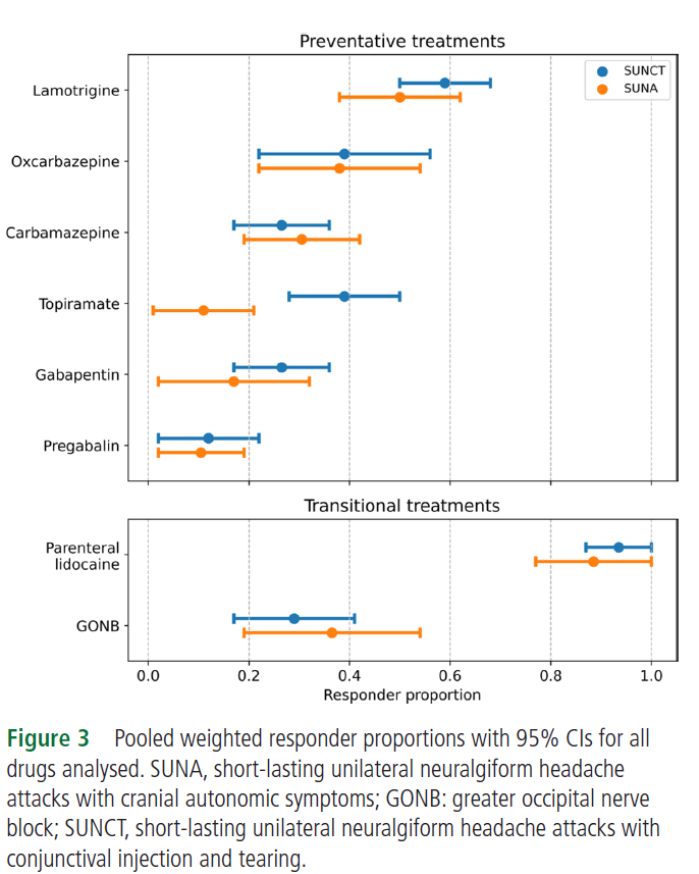
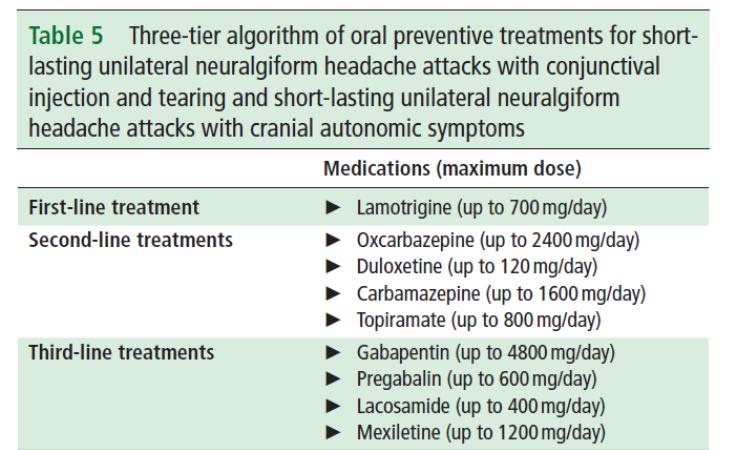
Treatment
- Lamotrigine,
Topiramate and gabapentin are moderately effective in prevention
- Lacodamide has been tried with some effect
- IV lidocaine
infusion – 90% respond, lasts mean 22 days
- GON block
- 38% respond,
lasts mean 41days