Tuberous
Sclerosis
Definition
Progressive, genetic disease characterised by:
• Hypopigmented macules of the skin
• Migrational errors of the brain
• Seizures
• Cognitive impairment
• Hamartomas of multiple organ systems including – skin, kidney, brain, lung, heart
Epidemiology
• 1/6800 to 1/17300
• Onset in infancy
• Autosomal dominant, M=F
• High spontaneous mutation rate, 40% familial, 60% sporadic
Aetiology
• Inactivation of either:
o TSC1 gene on chromosome 9q – encoding hamartin
o TSC2 gene on chromosome 16p – encoding tuberin
• Both protein part of a complex that is an important negative regular of mTOR pathway
• Mosaicism can occur
Diagnosis
• Genetic testing can identify mutations in 85-90% of patients
Cerebral imaging
CT
• Cortical tubers – Hypodense to isointense
o Calcification in most with age.
• SEN – calcification
• SEGA - Mixed density with moderate enhancement in most.
MRI
• Cortical tubers
o Adults – isointense to cortex on T1 (unless calcification), outer margin may be hyperintense and subcortical component hypointense
- Mixed signal on T2, deeper component more hyperintense
- Occasional contrast enhancement (3-5%)
• Subependymal nodules
o Small nodules protruding from the wall of lateral ventricles
o Change with age – in adults isointense with white matter
o Most calcify – seen on SWI, hypointense on T2
o Contrast enhancement variable, 50% show significant enhancement (does not indicate malignancy)
o Growth (>20%) on subsequent scans may indicate SEGA
• White matter lesions
o 100% of patients
o Streaky linear or wedge shaped lesions (T2 hyperintense in adults) along radial bands from the ventricles to the under surface of cortical tubers
o Small round syst-like lesions in 50% of patients – resemble CSF
• SEGA
o Most found around the foramen of Munro
o Mixed intensity on T1 and T2
o Nearly all enhance strongly
o Rarely invade brain
o Look for associated hydrocephalus
• Other
o Cerebellar tubers
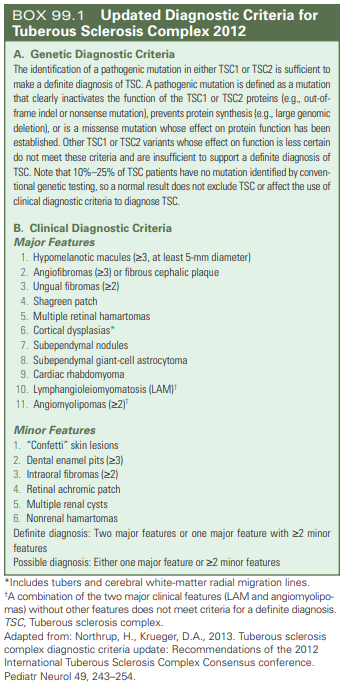
Clinical criteria:
Clinical manifestations
Neurological
Symptoms
• Intellectual
disability
• Epilepsy(80-90%)
o
Most onset in first year of life
o
Most common cause of infantile spasms
o
Treated with vigabatrin and ACTH
• Behavioural
abnormalities
o
Autism 25-50%
• Spectrum
from mild/no symptoms to severe
Pathology
• Cortical/subcortical
tubers
• White
matter abnormalities
• Subependymal
hamartomas (SEN)
o
Grow over time, usually only into adolescence –
then calcify
• Subependymal
giant cell astrocytoma (SEGA)
o
Transform from SEN
o
6-14% of patients
o
Usually benign but locally invasive
Renal
• Renal angiomyolipomas (75%)
o Most present by 10 years of age
• Renal cysts (20%)
Cardiac
• Rhabdomyomas (30-50%)
o Rarely symptomatic
- Can obstruct valves or disrupt conduction system
o Tend to regress after infancy
Dermatological
• Hypomelanotic macules (61-97%)
o A few mm up to several cm
o Oval, ‘ash-leaf’ shape
• Angiofibromas
o Adenoma sebaceum – small, red-pink skin lesions in butterfly pattern on the face, onset mid-late childhood in 70%
o Fibrous plaques
• Shagreen patches – thick, flesh coloured macules in the lumbosacral region
• Ungual fibromas and angiofibroma’s of the nailbed.
Pulmonary
• Lymphangiomyomatosis (LAM) - (24-49% of adult females)
o Onset ~30-35years, progressive
o Normal structure of the lungs replaced by multiple cysts
o Exacerbated by oestrogen
o Significant cause of mortality
Visual
• Retinal hamartoma (40-50%)
• May impair vision – most asymptomatic
Management and screening
mTOR inhibitors
• Everolimus and sirolimus
• (In Australia Everolimus is PBS subsidised for SEGA or visceral tumours)
• Demonstrated to reduce progression of disease in a number of organs
Screening and treatment considerations
|
|
Screening |
Treatment comments |
|
Brain |
Asymptomatic patients <25yrs – MRI
brain to monitor for SEGA – 1-3 years Known large or growing SEGA – MRI brain
– frequency is dependent on specific circumstances Infants up to 24 months - regular EEG’s
(even in asymptomatic) to detect early seizures. Patients >24 months - Consider EEG
if clinical or behavioural change Perform screening of TSC associated
neuropsychiatric disorders (e.g. Autism, ADHD, Anxiety, Depression) |
mTOR inhibitors can be considered for
enlarging or symptomatic SEGA Surgery or VP shunting for large SEGA Seizures may respond particularly well
to vigabatrin |
|
Renal |
MRI of abdomen every 1-3 years
- to assess for progression of angiomyolipoma and renal cystic disease Renal function - Annual |
Large (>4cm) lesions may need treatment
(surgery or ablation). mTOR inhibitors
may also help shrink renal lesions. |
|
Respiratory |
Females - Baseline HRCT chest in
all females at age 18 then every 5 years to menopause if asymptomatic (more
often if symptomatic or known lung disease) Male – At age 18 years if symptomatic
then only need repeat testing if known lung disease or new symptoms Respiratory function tests in any
patient with changes on imaging or symptoms.
VEGF levels can be measured to
monitor progress in affected patients. |
Avoid oestrogen exposure (note risk with
pregnancy) mTOR inhibitors can be considered for
symptomatic disease |
|
Heart |
Echo every 1-3 years in asymptomatic
paediatric patients or until regression of cardiac rhabdomyomas Frequency/necessity of Echo
monitoring unclear in adults (probably only if symptomatic or ECG
abnormality) Consider ECG ever 3-5 years in
asymptomatic patients |
Cardiac lesions rarely require
intervention and usually spontaneously regress. |
|
Skin |
Annual skin check |
Angiofibroma will respond to mTOR
inhibitors (generally cosmetic treatment) Avoid sun exposure which worsens
lesions. |
|
Dental |
Annual dental check (jaw/oral
fibromas) |
|
|
Eye |
Annual ophthalmic examination in childhood.
?Frequency in adulthood |
|